


매일미사
우리들의 묵상/체험
| 제목 | 20 11 05 (목) 평화방송 미사 코의 인두와 부비동을 집중적으로 다스려 귀안에 침 눈물 산소를 보내주고 압력을 다스려 조직 기관 청신경이 활발하게 움직임 | |||
|---|---|---|---|---|
작성자한영구

|
작성일2021-01-11 | 조회수1,532 | 추천수0 |
반대(1)
 신고
신고
|
|
성부와 성자와 성령의 이름으로 아멘. 흠숭 하올 삼위일체이신 우리 주님. 오늘 11월 5일 목요일 연중 제31주간 평화방송 낮 12시 15분을 선택하여 미사에 참례하였습니다. 미사 전에 가스를 토해내려고 하자 가스가 별로 나오지 않습니다. 하품도 하지 않고 바로 저의 입안의 침샘에서 침이 보통으로 솟아올라 그 침을 목구멍 위로 보내어 삼키었습니다. 요사이 저의 죄의 상처가 있는 곳에 상처를 치유하여주시고 빛의 생명을 주시어, 제안에 계신 하느님 뜻의 생명이 성장하고 발전하게 하여주십니다. 저의 생명도 동시에 성장하고 발전합니다. 공기의 물질대사를 다스려주시어 상처가 있는 혈관 안에 산소가 흘러들어 순환하게 하여주시고, 침의 물질대사를 다스려주시어 상처를 치유하여주신 효과가 나타나 이처럼 가스도 안 나오고 침만 조금 삼키게 하여주시니 감사합니다. 미사가 시작되자 저의 두 눈 사이 콧날 양쪽 경사 끝에 머물러 만져주십니다. 이어서 바로 저의 두정엽 정수리 가운데에 머물러 만져주시면서 빛의 생명을 아래 두 눈 사이 콧날 양쪽 끝과 연결하여 주십니다. 이어서 바로 저의 오른쪽 코의 물렁 코뼈 오른쪽 약간 위 경사 끝 뼈에 머물러 만져주십니다. 이 세 곳을 연결하여 빛의 생명을 주십니다. 아래 물렁 코뼈 오른쪽 약간 위 경사 끝 뼈 뒤에는 코의 인두 윗부분이 위치하여 그곳을 연결하여 침의 물질대사를 다스려주어 건조한 귀 안으로 침을 보내주십니다. 두 눈 사이에 머물러 벌집 굴과 연결하여 공기의 물질대사를 다스려 산소를 저의 오른쪽 귀 안에서 보내주고, 공기의 압력을 조절하여, 침, 산소, 압력이 조화롭게 작용하여, 크게 내이의 조직의 기관이 움직이는 소리가 계속 들립니다. 귀의 청력을 회복시켜 주십니다. 이어서 물렁 코뼈 오른쪽 약간 위쪽 경사 끝 뼈의 위치에 머물러 위턱뼈 굴과의 연결을 열어 그곳과 저의 오른쪽 눈썹 오른쪽 끝부분과 연결하여 그 아래에 있는 눈물샘의 눈물을 분비하여 그 눈물을 귀 안으로 흘러들게 하십니다. 침이 부족하므로 눈물까지 다스려주시어 산소, 침, 눈물, 압력이 조화롭게 작용하여 귀 안에서 내이의 조직의 기관이 활발하게 움직이는 소리가 들리도록 다스려주십니다. 이어서 저의 두정엽 정수리 가운데에 머물러 만져주시어 수직으로 빛의 생명을 주십니다. 저의 코의 인두 윗부분과 연결하여 침의 물질대사를 다스려 침을 귀 안의 건조한 조직과 기관으로 흘러들게 하십니다. 그리고 다시 저의 그 코의 인두 위쪽 뼈에서 저의 오른쪽 눈꺼풀과 연결하여 눈꺼풀 위에 머물러 만져주십니다. 눈꺼풀은 나비 굴 - 접형동 -과 연결되는 곳으로 시신경과 신경계에 산소를 공급하여 주신다고 상상합니다. 그리고 다시 저의 코의 인두의 위쪽 위치, 물렁뼈 코의 양쪽 약간 위의 경사 끝 뼈에서 V자형으로 저의 오른쪽 눈꺼풀을 거쳐서, 전두엽 우뇌 상단 오른쪽 끝에 머물러 연결하여 다스려주십니다. 그리고 두정엽 정수리 가운데에서 후두엽 머리털 가마와 연결하여 만져주시고 다시 정수리로 올라와 만져주시면서 강력한 빛의 생명을 주십니다. 침의 물질대사를 다스려주시어 침이 건조한 귀 안의 조직과 기관에 흘러들게 하여주십니다. 귀 안에서는 오른쪽 귀에서만 큰 소리로 내이의 조직의 기관이 활발하게 움직이는 소리가 들립니다. 제가 청력이 빨리 회복되지 않아 지금 불편을 겪고 있습니다. 그러므로 성령님께서 저의 청력을 회복시키기 위하여 모든 다스림을 그곳에 집중하십니다.
미사가 끝난 후에도 저의 물렁 코뼈 끝에서 오른쪽 약간 위쪽 경사 끝 뼈에 머물러 만져주십니다. 그곳은 저의 아래 눈꺼풀과 수평을 이루는 위치이므로 저의 아래 눈꺼풀에 머물러 오른쪽으로 옮겨가시면서 머물러 만져 주십니다. 머리 뒤통수 후두엽 하단에서 오른쪽 뼈끝 - 오른쪽에 귀 바퀴가 있음 -에 머물러 만져주시자 부비동 나비 굴과 연결이 이루어져, 그 눈꺼풀에 머물러 시신경과 청신경과 신경계와 연결하여 산소를 그곳에 공급하여 주신다고 상상합니다. 오늘 귀 안에서는 내이의 조직의 기관과 청신경에 산소가 공급되고, 침도 적당량을 공급하여 주시고 눈물까지도 보내주시어 완벽한 조화를 이루어 내이의 조직의 기관이 활발하게 움직이도록 다스려주시었습니다. 끝 무렵에는 시신경과 청신경과 신경계에도 연결하여 그곳에 산소를 혈관을 통하여 보내주시었다고 상상합니다. 오늘 1시간 가까이, 미사 전은 짧게, 미사는 처음부터 끝까지 계속 다스려주시고, 미사 후에도 이처럼 길게 다스려주시었습니다. 흠숭 하올 삼위일체이신 우리 주님. 오늘도 이 못난 작은 이를 사랑하여주시어 성령님께서 저의 귀 안에서 내이의 조직의 기관이 아주 큰 소리로 활발하게 움직이어 고막의 안쪽을 압력으로 두드리어 큰 소리가 들리도록 다스려주시었습니다. 저의 고질적으로 이 청력이 나빠진 것을 정상으로 회복시켜 주시기 위하여, 이처럼 다스려주시어 성장하고 발전한 저의 영혼과 몸과 그 다스려주시는 생명 지식을 좀 알게 하여주신 것과 이 모두를 주님께 바칩니다. 입술이 건조하여 침을 바릅니다. 거룩하신 하느님의 뜻으로 이 못난 작은 이를 사랑하시어 이처럼 다스려주시니 감사합니다. 주님을 더욱더 하느님 뜻의 사랑으로 사랑합니다. 아멘. 영광이 성부와 성자와 성령께 처음과 같이 이제 와 항상 영원히 아멘. 성부와 성자와 성령의 이름으로 아멘.
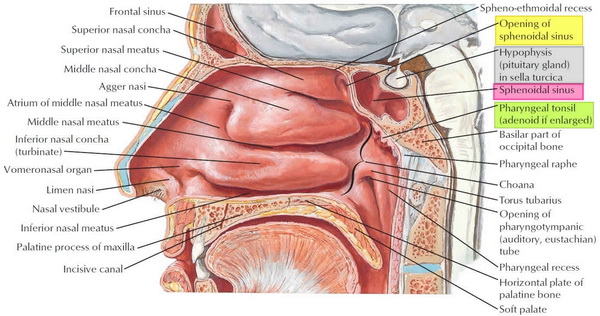 나비 굴 - 접형동 -의 구조 기능 감염 수술 출처 : Health Jade agger nasi : A small ridge on the lateral side of the nasal cavity. - 비강 옆면의 조그만 길죽 하게 솟은 부분 atrium of middle nasal meatus : 중비도(中鼻道) 안마당 vomeronasal organ : 보습 (保濕)코기관. 비서- 쥐- 기관 limen nasi : 코 문턱 .- 코문턱, 비역(鼻閾). 외측비연골과 대비익연골외측각(大鼻翼軟骨外側角)의 연결부에 있는 능(稜)으로서, 비강전정(鼻腔前庭)과 비강 자체 사이의 경계를 나타낸다. palatine process of maxilla ; 입 천장 – 구개-의 위 턱뼈 굴 열림 공정 incisive canal : 앞니 관 hypophisis (pituitary gland) in sella turcica : 말 안장 모양 안에 뇌하수체 pharyngeal tonsil (adenoid if enlarged) : 인두편도(임파선이 확장되었다면) basilar part occipital bone : 후두골의 두개골 밑부분 pharyngeal raphe : 인두(咽頭)(부근)의 봉선(縫線) choana : 후비공 torus tuberous ; 덩이줄기가 있는 원환체 opening of pharyngotympanic (auditory, eustachian) tube : 귀의 유스타키오관의 열림 pharyngeal recess : 인두(咽頭)(부근)의 휴식 horizontal plate of palatine bone : 구개(口蓋)골의 수평 판
접형동 -나비 굴 - 구조 기능 감염 수술 출처 : Health Jade 내용 [ 숨기기 ]
접형동 접형동 부비동 기능 접형동 감염 부비동염의 원인은 무엇입니까? 부비동염의 증상은 무엇입니까? 부비동염 진단 부비동염 치료 옵션 수술 접형동 수술 접형동 수술 기법 내시경 접형동 절개, 자연 연체동물의 심장에 있는 작은 구멍을 통한 Transnasal 내시경 접형동 절개, 자연 연체동물의 심장에 있는 작은 구멍을 통한 Transethmoidal 내시경 접형골 절개술, 전부 동벽을 통한 경종 절개술 접형동의 세척 접형 부비 동경 검사를 통한 비강 / 부비동 내시경 접형동 공의 확장을 동반 한 비강 / 부비동 내시경 접형동 수술 위험 접형동 수술 회복 접형동 수술 결과 접형동 접형동은 가장 후부 부비동입니다. 접형동은 접형골의 몸체 내에 형성된 쌍을 이루는 공간으로, 전벽의 접형골 오목 부를 통해 비강 지붕과 연결됩니다 (그림 1). 구멍은 접형동 부비동의 전벽에서 높습니다. 두 부비동은 중간 선에있을 수도 있고 없을 수도있는 중격으로 분리됩니다. 접형동은 보통 셀라보다 앞쪽에 있습니다.
큰 부비동은 인접한 구조와 관련된 다수의 융 기부와 함몰 부를 보여줄 수 있습니다. 여기에는 뇌하수체, 시신경 및 내 경동맥이 포함될 수 있습니다.
접형동 부비동 위치 : 접형동 뼈의 중앙 몸체는, 말안장. -접형골체(蝶形骨體)의 상면에서 정중선을 횡으로 가로지는 함요로서, 뇌하수체를 포함하고 있다.- 보다 앞쪽에 있습니다. 접형동 혈액 공급 : 후 사골 및 접형골 동맥 접형동 신경 분포 : 후 사골 신경과 날개 구개 신경절의 안와- 눈알이 박혀 있는 구멍 -가지 접형동은 관련이 있습니다.
두개강(頭蓋腔-머리뼈 안 공간) 위, 특히 뇌하수체와 시신경 교차까지, 측면으로, 두개강, 특히 해면 동(海綿洞)- 공간 속에 섬유 기둥이 얽혀 있고 그 사이에 혈액이 차 있는 공간. 음경 해면체굴과 요도 해면체굴이 있다. 출처: 우리말 샘. 해면 정맥동은 눈 뒤쪽의 두개저에 있는 대정맥입니다. 이 정맥은 얼굴의 혈관으로부터 혈액을 배출합니다. 해면 정맥동은 공기가 들어있는 코곁동굴(부비동)이 아닙니다. 그리고 아래와 앞, 비강까지. 뼈의 얇은 선반 만이 접형동을 아래의 비강과 위의 하강과 분리하기 때문에, 먼저 접형골의 전 하부 측면을 통과하여 접형동으로 통과하여 비강의 지붕을 통해 뇌하수체를 외과 적으로 접근 할 수 있습니다. 그리고 접형골의 꼭대기를 통해 하체 골로 들어갑니다.
접형동의 신경 지배는 다음에 의해 제공됩니다.
안과 신경의 후방 사골 분지 [V1]. 과 상악 신경 [V 2]은 날개 구개 신경절의 안와- 눈알이 박혀 있는 구멍 -가지를 통해 전달됩니다. 접형동은 상악 동맥의 인두 동맥 가지에 의해 공급됩니다.
처지
위 위치 : 해면 동, 후부 접형동 안장형의 함요(陷凹- 움푹 들어간)에 인접한 벽 안의 내용물 아래 위치 : 비강 전방 : 비강, 사골 후방 공기 세포 후방 : 중두 개와의 내용물 측면 : 해면 동, 두개강(頭蓋腔-머리뼈 안) 공압 화의 유형
기초 또는 부재 접형동 측면 홈 두꺼운 뼈에 의해 sella- 안장형의 함요 - 와 분리 된 후 접형동 벽 후부 접형동 (불완전하거나 완전 할 수 있음) 접형동 부비동은 임신 약 3 개월에 발달하기 시작하는 접형골의 중앙 통기입니다. 그들의 발달은 연골 컵 모양 과정의 질화로 시작되며 10 대까지 계속 확대됩니다.
접형동 기압의 높은 가변성으로 인해 경계가 사람마다 다를 수 있습니다.
접형동의 앞쪽 경계가 가장 일관적일 수 있습니다. 여기에는 사골 뼈의 수직 판과 연결되는 앞쪽 쐐기 모양의 문장과 보습 (保濕)코기관과 연결되는 앞쪽의 주둥이가 포함됩니다. 접형동의 후방 경계는 보통 중간에 팔라 터 시카와 옆으로 해면 동을 포함합니다.
Hamberger 1) 은 말안장. -접형골체(蝶形骨體)의 상면에서 정중선을 횡으로 가로지는 함요로서, 뇌하수체를 포함하고 있다.- 와의 관계에 따라 3 가지 유형의 공압 화를 설명했습니다 : conchal (기초 또는 부재 접형동), presellar (두꺼운 뼈에 의해 sella- 안장형의 함요 - 와 분리 된 후 접형동 벽) 및 sellar (후부 접형동) sella- 안장형의 함요(陷凹- 움푹 들어간)에 인접한 벽). 그의 시리즈에서 가장 일반적인 구성은 판매 전 유형 (11 %) 및 콘찰 유형 (3 %)에 비해 인구의 86 %에서 발견 된 판매 유형이었습니다.
저자들은 쐐기 형 부비동이 말안장. -접형골체(蝶形骨體)의 상면에서 정중선을 횡으로 가로지는 함요로서, 뇌하수체를 포함하고 있다.- 너머로 확장되어 접형동 지붕의 일부를 형성하는 매우 일반적인 네 번째 구성 인 postsellar 유형을 설명했습니다. 또한 시신경 교차와 내 경동맥은 접형동의 후방 또는 측벽과 밀접하게 관련되어 있습니다.
접형동의 측면 한계는 크게 다릅니다. 접형동의 하측 영역은 날개 신경을 전달하고, 상측 측 영역은 회전 공동에서 V2를 전달합니다.
접형동의 측면 범위는 이러한 신경까지 또는 그 이상으로 확장 될 수 있습니다. 접형 동 구개(口蓋) 동맥의 후방 중격 가지는 접형동의 자연적인 os 아래 몇 밀리미터 아래에 있습니다.
동맥 공급
후 사골 동맥 접형 동 구개(口蓋) 동맥의 비강 가지 정맥 배액
후 사골 정맥을 통한 상안 정맥 림프 배수
림프 배액은 후 인두 결절로 이어지는 구 심성 혈관을 통해 발생합니다. 신경 지배
부교감 신경 : 날개 구개 신경절의 안와 가지 감각 : 삼차 신경의 안과 분열의 한 가지 인 비골 신경의 후방 사골 신경 변형 해부학
시신경 관계와 관련하여 :
유형 1 : 접형동에 인접 유형 2 : 부비동 들여 쓰기 유형 3 : 부비동 횡단 유형 4 : 후 사골동에 인접 개발
공압 화는 약 2 세에 시작되며 다른 부비동보다 느리게 진행됩니다.
그림 1. 접형동
접형동 접형동 부비동 기능 부비동의 전체 기능은 명확하지 않습니다 2) . 공동은 상당한 질량을 추가하지 않고도 뼈 구조의 증가를 허용합니다. 또한 성별 및 성적 성숙과 같은 것을 나타내는 사회적 단서를 제공합니다. 호흡기 점막이 부비동을 감싸고 있습니다. 이 호흡기 점막은 섬모가되어 점액을 분비합니다.
접형동은 접 형체의 몸체에서 발견됩니다. 그들은 접 형상-민족 오목 부의 후벽으로 열립니다.
사골동은 궤도 사이에서 발견됩니다. 그들은 일반적으로 3에서 18까지의 숫자가 다양한 일련의 미로에 의해 형성됩니다.이 사골 공기 세포는 구멍의 위치에 따라 국소 적으로 전방, 중간 및 후방으로 나뉩니다. 전방 사골동은 사골 근 또는 전두 관으로 열립니다. 중간 그룹은 사골 수포로 열리거나 그보다 우월합니다. 후방 그룹은 상비도의 측벽으로 열립니다.
부비동 중 가장 큰 것은 상악동입니다. 얼굴의 상악에는 양측에 2 개의 피라미드 모양의 상악동이 있습니다. 상악의 질량을 줄이기 위해 뼈 전체를 채 웁니다. 상악동은 중비도의 측벽에서 발견되는 반달 열공의 중심으로 열립니다.
삼각형 모양의 전두동은 궤도보다 우수한 전두골에서 발견됩니다. 이 부비동은 크기가 다양합니다. 그들은 중도의 측면 벽에서 열리고 상악동을 배수하는 반달 열공으로 계속됩니다.
접형동 감염 부비동염은 미국 성인 8 명 중 1 명에 영향을 미치며 연간 3 천만 건 이상의 진단을받습니다. 3) . 비 부비동염이라고도하는 부비동염은 증상이 코와 부비동 모두를 포함하기 때문에 매년 성인 8 명 중 1 명에게 영향을 미칩니다. 많은 사람들에게 염증은 바이러스 나 박테리아가 부비동을 감염시킬 때 (종종 감기 동안) 시작되어 증식하기 시작합니다. 감염에 대한 신체 반응의 일부로 인해 부비동 내막이 부풀어 오르고 부비동을 배출하는 채널이 차단됩니다. 이것은 점액과 고름이 코와 부비동을 채우게합니다. 다른 사람들에게는 증상과 염증이 환경의 다른 것들에 반응하는 코와 부비동의 결과 일 수 있지만 감염은 아닙니다.
부비동염은 단순히 부비동의 염증을 의미하기 때문에 단어만으로도 다양한 유사한 문제가 포함됩니다. 급성 부비동염은 증상이 4 주 미만 동안 나타나는 경우입니다. 만성 부비동염 진단을 받으려면 증상이 12 주 이상 지속되어야합니다. 때때로 이들은 동일한 원인으로 인해 발생하지만 종종 만성 및 급성 부비동염은 서로 매우 다릅니다. 주치의 또는 이비인후과 (귀, 코, 인후) 전문의 또는 이비인후과 전문의가 귀하의 부비동염 유형과 치료 방법을 파악하는 데 도움을 줄 수 있습니다. 재발 성 급성 부비동염은 누군가가 1 년 동안 4 번 이상의 부비동 감염 (급성 부비동염)을 앓 았지만 감염 사이에 증상이없는 경우입니다.
네 가지 부비동염 분류 :
급성 비 부비동염 : 갑작스런 발병, 완전한 해결로 4 주 미만 지속. 아 급성 비 부비동염 : 급성 비 부비동염의 연속이지만 12 주 미만입니다. 재발 성 급성 비 부비동염 : 1 년의 기간에 각각 최소 7 일 동안 지속되는 4 회 이상의 급성 에피소드. 만성 비 부비동염 : 증상의 징후가 12 주 이상 지속됩니다. 부비동염의 원인은 무엇입니까? 급성 부비동염은 가장 일반적으로 바이러스 나 박테리아로 인해 발생하며 일반적으로자가 제한적입니다. 감기에 걸린 환자의 약 90 %는 바이러스 성 부비동염을 가지고 있습니다. 급성 바이러스 성 부비동염은 10 일 미만 동안 아프고 악화되지 않는 경우에 발생할 수 있습니다. 급성 세균성 부비동염은 병에 걸린 후 10 일 이내에 전혀 호전되지 않거나 호전되기 시작한 후 10 일 이내에 악화되는 경우입니다. 아토피 (알레르기)가있는 사람은 일반적으로 부비동염에 걸립니다. 알레르겐, 자극제, 바이러스, 곰팡이 및 박테리아에 의해 발생할 수 있습니다. 인기있는 자극제는 동물의 비듬, 오염 된 공기, 연기 및 먼지입니다.
그러나 만성 부비동염은 일반적으로 장기간 감염이 아닌 장기간의 염증으로 인해 발생합니다. 감염은 만성 부비동염의 일부일 수 있으며, 특히 때때로 악화 될 때 발생하지만 일반적으로 주요 원인은 아닙니다. 정확한 원인을 항상 확인할 수있는 것은 아닙니다. 어떤 이유로 코와 부비동이 감염이라고 생각하는 것에 과도하게 반응합니다.
남부, 중서부 및 여성에서 부비동염의 비율이 더 높습니다. 15 세 미만의 어린이와 25 ~ 64 세의 성인이 가장 많이 영향을받습니다 . 4) .
다른 위험 인자 또는 부비동염 포함 ) 5 :
중격 이탈, 폴립, 중비갑개(中鼻甲介)의 낭포성 확장. 기타 외상 및 부비동 또는 주변 안면 부위와 관련된 골절과 같은 해부학 적 결함 낭포 성 섬유증, 섬모 운동 이상증과 같은 질병으로 인한 점액 수송 장애 화학 요법, HIV, 당뇨병 등으로 인한 면역 결핍 점액 섬모 청소를 손상시키는 장시간 앙와위 자세로 인한 신체 위치, 중환자 실 (ICU) 환자. 약물 비염, 독성 비염, 코코 카인 남용, 압력 외상, 이물질 점막 내막 건조로 인한 장기간 산소 사용 비위 관 또는 비 기관 관이있는 환자 관련된 조건이나 합병증이 있습니까?
편두통이나 긴장성 두통은 부비동 통증이나 압박의 증상을 유발할 수 있습니다. 변색 된 배액이없는 부비동 두통이있는 경우, 편두통 두통이 부비동 통증이나 압박을 유발할 가능성과 편두통 치료를위한 약물 옵션에 대해 주치의 또는 ENT 전문가에게 문의하십시오. 때때로 비강의 염증은 또한 배액과 비강 혼잡을 유발할 수 있지만 부비동과 관련이 없습니다.
부비동염의 증상은 무엇입니까? 최대 4 주 동안 코에서 배액이 흐리거나 유색인 경우 급성 부비동염과 다음 증상 중 하나 이상이 나타납니다.
코 막힘, 막힘, 막힘 얼굴, 머리 또는 눈 주위의 통증, 압박 또는 충만 오래 지속되는 감기 증상 병이 난 후 10 일 이내에 개선되지 않거나 처음에는 나아졌다가 다시 악화되는 증상 최소 12 주 동안 아래 4 가지 증상 중 2 가지 이상이 있으면 만성 부비동염이있을 수 있습니다. 이비인후과 전문의는 또한 만성 부비동염을 완전히 진단하기 위해 폴립, 고름 또는 코의 두꺼워 진 점액을 보거나 CT 스캔을 받아야합니다. 가능한 증상은 다음과 같습니다.
코가 막히거나 막힌 물건 얼굴, 머리 또는 눈 주위의 통증, 압박 또는 충만 두꺼워 진 비강 배액 후각 상실 부비동염 진단 진단은 일반적으로 임상 적이므로 급성 단순 부비동염에 대한 실험실 검사는 표시되지 않습니다. 부비동염의 증상 (방출 + 압력 또는 막힘)이있는 경우 부비동염의 단순 부비동염을 진단하기 위해 부비동의 X- 레이 또는 CT 스캔이 필요하지 않습니다. 단순 부비동 X- 레이는 상악, 전두엽 또는 접형골 질환에 대해 가장 정확하지만 대부분의 부비동 질환이 발생하는 앞사골 세포 또는 오스 티노 마티스 복합체를 평가하는 데 유용하지 않습니다. 일반 필름에서 긍정적 인 결과는 공기 유동 수준, 부비동 불투명도 또는 6mm 이상의 점막 비후입니다. 3mm ~ 4mm 두께의 Coronal CT가 선택 양식입니다. 부비동염을 시사하는 CT 소견은 부비동 혼탁, 기류 수준, 부비동 벽 변위 및 4mm 이상의 점막 비후입니다.
부비동염 치료 옵션 부비동염은 원인에 따라 다르게 치료됩니다. 대부분의 급성 부비동염 사례 ( 약 98 %)는 박테리아가 아닌 바이러스에 의해 발생하므로 항생제로 치료해서는 안됩니다. 급성 바이러스 성 부비동염은 아세트 아미노펜 또는 이부프로펜, 스테로이드 비강 스프레이 또는 코의 염수 관개와 같은 진통제를 사용하여 치료할 수 있습니다. 이러한 치료는 또한 급성 세균성 부비동염에 대한 좋은 옵션입니다. 대부분의 사람들은 "감시 대기"라고하는 급성 세균성 부비동염에서 자연적으로 좋아 지지만, 일부 급성 세균성 부비동염 환자는 항생제를 사용하면 더 빨리 좋아질 수 있습니다.
항생제 :저항의 커뮤니티 패턴을 기반으로 경험적으로 사용하십시오. 아목시실린 또는 아목시실린-클라 불라 네이트 10 ~ 14 일이 1 차 치료입니다. 일부 지역 사회에서는 아목시실린 효과가 70 % 미만입니다. Trimethoprim-sulfamethoxazole은 일부에 잘 맞지만 저항률이 더 높습니다. 치료 7 일 후 증상이 해결되지 않으면 어그 멘틴, 세푸 록심 악세 틸, 기타 2 세대 또는 3 세대 세 팔로 스포린, 클린다마이신 단독 또는 시프로플록사신, 설파 메톡 사졸과 함께 10 ~ 14 일 간의 더 넓은 스펙트럼 제제로 전환해야합니다. 마크로 라이드, 또는 플루오로 퀴놀론 중 하나. Metronidazole은 혐기성 적용 범위를 증가시키기 위해 이러한 약제 중 하나에 첨가 될 수 있습니다. 만성 부비동염의 경우 항생제가 S. 구균은 만성 질환에서 흔히 발생하는 베타-락타 마제 생성 유기체의 높은 발생률에 대해 효과적입니다. 환자가 5 ~ 7 일 후에도 호전되지 않으면 메트로니다졸 또는 클린다마이신을 추가하십시오. 3 ~ 6 주 동안 치료하십시오.
기류 수치가있는 정면 또는 접형 부비동염은 정맥 내 (IV) 항생제로 입원해야 할 수 있습니다. 면역력이 약하거나 독성이있는 환자는 입원이 필요합니다. 곰팡이 부비동염은 높은 이환율과 사망률과 관련이 있습니다.
부비동염은 얼굴과 궤도의 뼈와 연조직까지 확장 될 수 있습니다. 안면 봉와직염, 안와 주위 봉와직염, 안와 농양 및 실명이 발생할 수 있습니다. 부비동염은 해면 동 혈전증, 경막 외 또는 경막 하 농흉, 수막염과 같은 두개 내 합병증을 유발할 수 있습니다.
만성 부비동염 은 급성 부비동염과 다르게 치료됩니다. 만성 부비동염은 감염보다 염증에 의해 더 많이 발생하기 때문에 만성 부비동염 치료는 염증을 조절하는 것을 목표로합니다. 염수 비강 관개 및 / 또는 비강 스테로이드 스프레이는 만성 부비동염 증상의 주요 치료법입니다. 항생제가 때때로 도움이 될 수 있지만 항상 그런 것은 아닙니다.
알레르기, 비강 폴립, 천식 및 감염과 싸우는 신체 능력 문제를 포함한 다른 요인은 부비동염과 함께 진행되어 치료를받지 않으면 악화 될 수 있습니다.
항히스타민 제는 초기 알레르기 성 부비동염에서만 효과가 있습니다. 국소 스테로이드는 비점막 부종을 감소시키는 데 사용되지만 만성 및 알레르기 성 부비동염에 더 효과적입니다. 세균성 질병이 강하게 의심되는 경우에만 항생제를 시작하십시오.
수술 드문 경우를 제외하고는 급성 부비동염의 경우 수술을 권장하지 않습니다. 때때로 부비동 감염이 눈, 얼굴 또는 뇌로 퍼질 수 있습니다. 이것은 응급 상황으로 간주되며 감염을 되돌리고 확산을 막기 위해 수술이 필요할 수 있습니다.
만성 부비동염의 경우 약물 및 기타 치료로 증상을 제어 할 수없는 경우 수술이 옵션입니다. 부비동 수술의 가장 일반적인 유형은 내시경 부비동 수술입니다. 연필 크기의 내시경 (내시경)을 사용하여 코와 부비동 내부를보고 수술을 안내합니다. 이 수술은 부비동과 코 사이의 자연적인 배액 경로를 넓혀 점액이 부비동에서 빠져 나가 공기가 들어올 수 있도록합니다. 스프레이와 관개와 같이 코와 부비동으로 전달되는 약물도 부비동에 더 잘 들어갈 수 있습니다. 수술 후.
풍선 부비동 늑골 확장은 내시경도 사용되는 새로운 치료 옵션이지만 부비동을 막고있을 수있는 뼈와 조직을 조심스럽게 제거하는 대신 풍선을 사용하여 부비동 개구부를 더 크게 만듭니다. 풍선 확장은 모든 유형의 만성 부비동염에 적합하지 않을 수 있으며 모든 부비동에 사용할 수는 없지만 상황에 따라 도움이 될 수 있습니다.
접형동 수술 접형골 절개술은 접형동 부비동의 외과 적 개통으로 일반적으로 전신 마취하에 시행됩니다. 외과의가 수술실이나 사무실 환경에서 국소 마취하에 접형 절개술을 시행하는 경우는 드뭅니다. 접형골 절개술의 적응증에는 의학적 치료에 불응 성인 급성 및 만성 접형 부비동염; 접형 종괴 또는 병변; 내 비골 두개골 기저 또는 뇌하수체 수술; 접형 형 뇌척수액 누출 복구; 내 비강 날개 신경 절제술; 및 시신경 또는 안와 감압 6) .
접형동 수술에는 절대 금기 사항이 없습니다. 상대적 금기 사항에는 전신 마취를 제한하는 동반 질환이나 출혈 위험을 증가시키는 상태가 포함됩니다. 내 경동맥 또는 시신경의 열개가있는 저형성 접형동 또는 접형동 강에 수술을 수행 할 때도주의해야합니다.
절차 계획
수술 전 영상에는 접형동의 뼈 구조 및 공압 화 패턴에 대한 정보를 제공하기 위해 부비동의 비 조영 CT 스캔이 포함되어야합니다. 관리되는 특정 질병에 따라 다른 영상 검사가 권장 될 수 있습니다. 접형골 절개술을 수행하기 전에 접형동과 관련하여 평가해야하는 특성은 다음과 같습니다.
말안장. -접형골체(蝶形骨體)의 상면에서 정중선을 횡으로 가로지는 함요로서, 뇌하수체를 포함하고 있다.- (conchal, presellar, sellar, postsellar)와 관련된 공압 화 패턴 자연 소공의 위치와 상 비갑개와의 관계 (아래 이미지는 상 비갑개 내측에 위치한 오른쪽 접형동 자연 소공을 보여줍니다). 뼈 열개 유무에 특히주의를 기울인 시신경, 시신경 교차 및 내 경동맥의 위치 후 사골 (Onodi) 세포의 존재 또는 부재. 합병증 예방
접형 절개술을 시행하기 전에 외과의는 환자의 해부학 적 변형과 부비동염의 정도를주의 깊게 검사해야합니다. 외과의는 접형동으로 안전하게 들어갈 수있는 표준 접근 방식을 사용해야합니다. 정당한 경우 정위 탐색을 고려해야합니다. 심각한 합병증을 피하기 위해 외과의는 의도하지 않은 두개골 기저부 손상으로 인한 뇌척수액 누출, 시신경 손상으로 인한 실명, 쐐기 형 동맥의 후 중격 분지에서 발생한 출혈 또는 내부 경동맥의 치명적인 출혈과 같은 잠재적 인 함정을 인식해야합니다. 동맥.
수행 된 기술에 관계없이 중요한 구조를 피하기 위해주의를 기울여야합니다. 시신경은 접형동 근처 또는 오노 디 세포 내에서 측면으로, 때로는 상부로 횡단 할 수 있습니다. 경동맥, 시신경 교차, 해면 동 또는 뇌하수체에 손상을 줄 수 있으므로 접형동의 후벽을 방해하지 않도록 특히주의해야합니다. 또한, 외과의는 접형동 동맥의 후 중격 분지가 접형동의 본질보다 열등하다는 것을인지해야합니다. 따라서 뼈와 점막을 열등하게 제거하면이 동맥에 부주의 한 손상이 발생하여 비 출혈이 발생할 수 있습니다. 이 동맥의 손상을 방지하는 몇 가지 방법은 하 절개를 수행하기 전에 뼈에서 점막을 높이거나 동맥의 대략적인 부위를 소작하는 것입니다.
접형동 수술 기법 몇 가지 특정 쐐기 형 절차를 수행 할 수 있습니다. 접형동 세척 및 진단 부비 동경 검사를 포함한 일부 절차는 접형동 절개 수술없이 접형동에 대한 접근을 제공합니다. 접형 공공의 외과 적 확장은 조직을 제거하지 않고 부비동 공공을 넓히기위한 최소 침습적 접근입니다 7) .
접형골 절개술은 접형동 부비동을 수술하는 수술입니다. 나비굴 절개는 조직 제거없이 또는 조직 제거와 함께 수행 할 수 있습니다. "조직 제거"라는 명칭은 점액이나 고름을 흡입하는 것이 아니라 물질이나 조직을 제거하는 것으로 American Academy of Otolaryngology-Head and Neck Surgery에 의해 정의되었습니다.
내시경 접형 절개술을위한 기술은 (1) 벌집 굴을 경유하는 접근 방식과 비강(鼻腔)을 경유하는 접근 방식과 (2) 자연 os를 통한 개방 대 전방 부비동 벽을 통한 개방으로 나눌 수 있습니다.
접형골 절개술의 크기 제한은 접형동의 크기에 따라 다릅니다. 접형골 절개술의 최적 크기는 알려져 있지 않습니다. 그러나 일반적으로 폴립 증 및 알레르기 성 진균 성 부비동염과 같은 폐쇄성 부비동 질환에서 더 넓은 접형 종을 수행하는 것이 중요하다고 간주됩니다. 접형동을 통한 확장 된 내 비강 접근은 종종 수반되는 후방 중격 절제술, 부비동 간 중격 제거, 주둥이의 일부와 전 접형동 벽의 하부 부분을 드릴링하는 등 확장 된 절차를 필요로합니다.
내시경 접형동 절개, 연체동물의 심장에 있는 작은 구멍을 통하여 비강을 경유하는 접근 방식 고립 된 접형동 질환 8)의 경우, 자연 공공을 통한 내시경적 비내 사골 - 벌집 굴 -절제 없이 내시경 비강 접형골 절제술을 고려할 수 있습니다 . 이 접근법은 코 점막을 최소한으로 파괴한다는 장점이 있으며 수술 및 회복 시간을 단축 할 수 있습니다. 그러나 사골 동강이 열리지 않았기 때문에 수술 후 접형 절개 부위에 대한 접근이 제한 될 수 있습니다.
30 ° 비강 내시경은 접형동 입구를 시각화하는 데 종종 유용합니다. 소공에 접근하고 수술 후 관리 및 검사를 용이하게하기 위해 상부 비갑개 부분을 제거해야 할 수 있습니다. 접형동의 자연 공공은 보통 상 비갑개 바로 뒤쪽에 있습니다. 접형동 부비동의 자연 공공을 찾는 데 사용할 수있는 해부학 적 지표는 다음과 같습니다. 9) :
접형골 오목 부에서 상 비갑개 뒤쪽; 자연 소공은 80 % 사례에서 상 비갑개의 중간입니다. 비강 바닥에서 30 ° 각도로 비강에서 약 6cm choana의 상부 연장 부에서 약 1cm 위 상악동 지붕의 대략적인 수준에서 접형 소공이 확인되면 접형동 버섯 펀치 또는 작은 Kerrison 펀치를 사용하여 확대합니다. 접형동 내부의 내용물은 배양, 생검, 관개 또는 제거됩니다. 내 경동맥, 시신경 또는 두개골 기저에 손상을 줄 수있는 접형동의 후벽을 조작하지 않도록주의해야합니다.
내시경 접형동 절개, 자연 연체동물의 심장에 있는 작은 구멍을 통한 벌집 굴을 경유하는 내시경 경종 절개술은 내시경적 비내 사골절제술 -의 통로를 통해 수행되는 접형 절개술입니다. 이 접근법은 파피 라 세아 박판에서 주둥이까지 접형동의 가장 넓은 시야를 제공하기 때문에 가장 일반적으로 수행되는 방법입니다. 접형동, 두개골 기저부 및 상 비갑개의 앞면이 식별 될 때까지 전체 민족지 절제술을 먼저 수행합니다. 그런 다음 자연 OS를 통해 또는 접형동의 앞면 뼈의 얇은 부분에 구멍을 뚫어 접형골에 접근하도록 결정할 수 있습니다. 이 두 가지 방법을 평가 한 비교 시험은 없지만 각각 이론적 및 일화적인 장점과 단점이 있습니다.
접형골 절개술을 자연 OS를 통해 수행하는 것은 수술 후 점액의 재순환을 제한하도록 이론화되었으며 접형동이 알려진 부비동을 통해 열리기 때문에 더 안전 할 수 있습니다. 반대로, 전부 동벽을 통한 접형골 절개술은 잠재적으로 건강한 상 비갑개를 제거하는 것을 방지하고 후각 기능 장애의 위험을 줄일 수 있습니다. 이 두 절차 사이의 비교 합병증과 개통 률은 알려져 있지 않습니다.
일반적으로 0 ° 비강 내시경이 시술에 사용됩니다. 각진 내시경 (30 °, 45 ° 또는 70 °)은 접형 절개술이 수행 된 후 큰 접형동 강의 모서리 또는 바닥을 시각화하는 데 때때로 사용됩니다. 자연 소공을 식별 할 때, 상부 비갑개의 1/3에서 절반까지의 하부는 종종 직선 절단 겸자를 사용하여 절제됩니다. 뇌척수액 누출로 인한 후각 기능 장애 및 두개골 기저 손상의 위험 때문에 상 비갑개를 너무 우월하게 절제하는 것은 바람직하지 않습니다. 접형동의 자연 공공은 보통 상 비갑개 바로 뒤쪽에 있습니다. 접형골 동 자연 소공을 찾기 위해 사용될 수있는 해부학 적 경계표는 다음과 같다 10) :
접형골 오목 부에서 상 비갑개 뒤쪽; 자연 소공은 80 % 사례에서 상 비갑개의 중간입니다. 비강 바닥에서 30 ° 각도로 비강에서 약 6cm choana의 상부 연장 부에서 약 1cm 위 상악동 지붕의 대략적인 수준에서 J- 큐렛 또는 이미지 유도 프로브는 처음에 시각화 할 수 없을 때 OS를 뭉툭하게 촉지하고 식별하는 데 도움이됩니다 . 11) . 자연 OS가 확인되면 곧은 버섯 펀치, Kerrison 펀치 또는 기타 도구를 사용하여 개구부를 측면 및 위쪽으로 확대 할 수 있습니다.
내시경 접형골 절개술, 전부 동벽을 통한 경종 절개술 전방 부비강 벽을 통한 내시경 경종 상 접형골 절개술은 잠재적으로 건강한 상 비갑개 제거를 방지하고 후각 기능 장애의 위험을 줄일 수 있습니다.
접형동, 두개골 기저부 및 상 비갑개의 앞면이 식별 될 때까지 전체 민족지 절제술을 먼저 수행합니다. 일반적으로 0 ° 비강 내시경이이 접근법에 사용됩니다. 각진 내시경 (30 °, 45 ° 또는 70 °)은 접형 절개술이 수행 된 후 큰 접형동 강의 모서리 또는 바닥을 시각화하는 데 사용할 수 있습니다.
상 비갑개는 일반적으로 외과의가 자연 OS를 통합하기로 결정하지 않는 한 절제되지 않습니다. 영상 안내 시스템은 부비동에 들어가기위한 안전한 위치를 찾는 데 사용될 수 있습니다. 이미지 안내를 사용할 수없는 경우 외과의는 두개골 기저 손상을 방지하기 위해 다소 열등하고 내측에 뚜렷하고 얇은 뼈가있는 위치를 선택해야합니다. 무딘 낫 칼 또는 J- 큐렛을 사용하여 접형동의 앞면에있는 얇은 뼈 부분을 뚫습니다. 접형동 버섯 펀치, Kerrison 펀치 또는 기타기구를 사용하여 접형골 절개술을 넓힐 수 있습니다.
접형동의 세척 접형동의 최소 침습적 절차는 접형동의 세척이며, 접형동은 자연 개구부를 통해 또는 접형동면을 통해 접근됩니다. 부비동은 식염수로 관개하고 흡인합니다. 그런 다음 병리학자가 내용물을 배양하거나 평가할 수 있습니다.
접형 부비 동경 검사를 통한 비강 / 부비동 내시경 sphenoid sinuscopy로 진단하는 비강 / 부비동 내시경은 천자가 생성되거나 비수술 적으로 열린 공공에 캐 뉼러를 삽입하는 절차입니다. 그런 다음 내용물을 관개, 흡인, 배양 또는 생검 할 수 있습니다.
접형동 공의 확장을 동반 한 비강 / 부비동 내시경 접형동 소공을 확장하는 비강 / 부비동 내시경은 접형동 소공을 기계적으로 확장하여 배액과 접형동에 대한 접근을 개선하는 절차입니다. 절차는 사무실 설정이나 수술실에서 수행 할 수 있습니다. 국소 마취 및 충혈 제거가 수행됩니다.
수술되지 않은 부비동에서 자연 소공은 일반적으로 상 비갑개 내측에서 식별됩니다. 사용되는 카테터의 스타일에 따라 프로브 또는 와이어가 소공에 부드럽게 삽입됩니다. 부비동이 성공적으로 삽관되면 팽창 장치 또는 풍선이 부비동 공으로 진행됩니다. 그런 다음 풍선을 부풀려 부비동 공을 확장합니다. 그런 다음 부비동 내용물을 관개, 흡인, 배양 또는 생검 할 수 있습니다.
접형동 수술 위험 내시경 접형 절개술의 위험은 다음을 포함하지만 이에 국한되지 않습니다 12) :
출혈 감염 마취 위험 흉터 질병의 재발 두개골 기저부 손상, 뇌척수액 누출 및 수막염 눈 또는 시력 상실 및 안와 신경 또는 시신경 교차 손상 경동맥 손상 수술 후 골 협착증 점막 형성 접형동 수술 회복 내시경 접종 절개술의 수술 후 관리는 기능적 내시경 부비동 수술의 다른 절차와 유사합니다. 환자는 종종 비강 식염수 관개 또는 세척을 하루에 여러 번 수행하도록 요청받습니다. 수술 후 항생제와 경구 용 코르티코 스테로이드는 의사의 선호에 따라 제공됩니다.
환자는 일반적으로 수술 후 약 1-2 주에 비강 내시경 검사를 위해 클리닉에서 debridement가 있습니다. 딱지와 혈전의 파편 제거와 흉터 조직의 조기 식별은 수술 후 유착을 제한하는 데 도움이됩니다.
접형동 수술 결과 접형동 절개는 사례 시리즈 연구 13) 에 근거하여 효과적입니다 . 접형 절개술을 평가 한 전향 적 무작위 대조 시험은 없습니다.
Sphenoid sinus
Contents [hide]
Sphenoid sinus Sphenoid sinus function Sphenoid sinus infection What causes sinusitis? What are the symptoms of sinusitis? Sinusitis diagnosis Sinusitis treatment options Surgery Sphenoid sinus surgery Sphenoid sinus surgery technique Endoscopic Sphenoidotomy, Transnasal via the Natural Ostium Endoscopic Sphenoidotomy, Transethmoidal via the Natural Ostium Endoscopic Sphenoidotomy, Transethmoidal via Anterior Sinus Wall Lavage of the sphenoid sinus A nasal/sinus endoscopy with sphenoid sinuscopy Nasal/Sinus Endoscopy, with dilation of sphenoid sinus ostium Sphenoid sinus surgery risks Sphenoid sinus surgery recovery Sphenoid sinus surgery outcomes
Sphenoid sinus The sphenoid sinus is the most posterior paranasal sinus. The sphenoid sinuses are paired spaces formed within the body of the sphenoid bone, communicating with the roof of the nasal cavity via the sphenoethmoidal recess in its anterior wall (Figure 1). The apertures are high on the anterior walls of the sphenoid sinuses. The two sinuses are separated by a septum which may or may not be in the midline. The sphenoid sinus usually lies anteroinferior to the sella.
A large sinus can show a number of ridges and depressions related to closely adjacent structures. These can include the pituitary gland, optic nerve and internal carotid artery.
Sphenoid sinus location: the central body of the sphenoid bone anteroinferior to the sella turcica Sphenoid sinus blood supply: posterior ethmoidal and sphenopalatine arteries Sphenoid sinus innervation: posterior ethmoidal nerve and orbital branch of pterygopalatine ganglion The sphenoidal sinuses are related:
above to the cranial cavity, particularly to the pituitary gland and to the optic chiasm, laterally, to the cranial cavity, particularly to the cavernous sinuses, and below and in front, to the nasal cavities. Because only thin shelves of bone separate the sphenoidal sinuses from the nasal cavities below and hypophyseal fossa above, the pituitary gland can be surgically approached through the roof of the nasal cavities by passing first through the anteroinferior aspect of the sphenoid bone and into the sphenoidal sinuses and then through the top of the sphenoid bone into the hypophyseal fossa.
Innervation of the sphenoidal sinuses is provided by:
the posterior ethmoidal branch of the ophthalmic nerve [V1] . and the maxillary nerve [V 2] via orbital branches from the pterygopalatine ganglion. The sphenoidal sinuses are supplied by branches of the pharyngeal arteries from the maxillary arteries.
Relations
superiorly: cavernous sinus, sella turcica and its contents inferiorly: nasal cavities anteriorly: nasal cavities, posterior ethmoid air cells posteriorly: contents of the middle cranial fossa laterally: cavernous sinus, cranial cavity Types of pneumatization
conchal lateral recess presellar sellar (which can be incomplete or complete) The sphenoid sinuses are central aerations of the sphenoid bone that start developing at about 3 months’ gestation. Their development initiates as a vagination of the cartilaginous cupular process and continues to enlarge until the teenaged years.
Because of the high variability of sphenoid sinus pneumatization, the boundaries can differ from person to person.
The anterior boundaries of the sphenoid sinus are likely the most consistent. They include the sphenoid crest anterosuperiorly, which articulates with the perpendicular plate of the ethmoid bone, and the rostrum anteroinferiorly, which articulates with the vomer. The posterior boundaries of the sphenoid sinus usually include the sella turcica medially and cavernous sinuses laterally.
Hamberger 1) described 3 types of pneumatization based on its relationship to the sella turcica: conchal (rudimentary or absent sphenoid sinus), presellar (a posterior sphenoid sinus wall that is separated from sella by thick bone), and sellar (a posterior sphenoid sinus wall that is adjacent to sella). The most common configuration in his series was the sellar type, found in 86% of the population, compared to the presellar type (11%) and conchal type (3%).
Authors have described a quite common fourth configuration, postsellar type, in which sphenoid sinus extends beyond the sella turcica so that the sella forms a portion of the roof of the sphenoid sinus. In addition, the optic chiasm and internal carotid arteries are often intimately associated with posterior or lateral walls of sphenoid sinus.
The lateral limits of the sphenoid sinus vary greatly. The inferolateral area of the sphenoid sinus carries the vidian nerve, and the superolateral area carries V2 in foramen rotundum.
The lateral extent of the sphenoid sinus may extend to or beyond these nerves. The posterior septal branch of the sphenopalatine artery runs a few millimeters below the natural os of the sphenoid sinus.
Arterial supply
posterior ethmoidal artery nasal branches of the sphenopalatine artery Venous drainage
superior ophthalmic veins via posterior ethmoidal veins Lymphatic drainage
Lymph drainage occurs via afferent vessels leading into the retropharyngeal nodes Innervation
parasympathetic: orbital branches of the pterygopalatine ganglion sensory: posterior ethmoidal nerve from the nasociliary nerve, a branch of the ophthalmic division of the trigeminal nerve Variant anatomy
With respect to optic nerve relationship:
type 1: adjacent to sphenoid sinus type 2: indenting the sinus type 3: traversing the sinus type 4: adjacent to posterior ethmoid sinus Development
Pneumatization starts at around 2 years of age and it develops more slowly than the other paranasal sinuses.
Figure 1. Sphenoid sinus
sphenoidal sinus Sphenoid sinus function The total function of the paranasal sinuses is unclear 2). The cavities allow for the increase in the bony structure without adding significant mass. They also provide social cues that indicate such things as gender and sexual maturity. Respiratory mucosa lines the paranasal sinuses. This respiratory mucosa is ciliated and secretes mucus.
The sphenoidal sinuses are found in the body of the sphenoid. They open into the posterior wall of the sphenoid-ethmoidal recess.
The ethmoid sinuses are found between the orbits. They typically are formed by a series of labyrinths which vary in number from 3 to 18. These ethmoidal air cells are divided regionally into anterior, middle and posterior, based on the location of their apertures. The anterior ethmoidal sinus opens into the ethmoidal infundibulum or the frontonasal duct. The middle group opens into the ethmoidal bulla or just superior to it. The posterior group opens onto the lateral wall of the superior nasal meatus.
The largest of the paranasal sinuses is the maxillary sinus. There are 2 pyramidal-shaped maxillary sinuses located bilaterally in the maxilla of the face. It fills the bone in its entirety to reduce the mass of the maxilla. The maxillary sinus opens into the center of the semilunar hiatus found in the lateral wall of the middle nasal meatus.
The triangular-shaped frontal sinuses are found in the frontal bone superior to the orbits. These sinuses vary in size. They open at the lateral wall of the middle meatus which then continues as the semilunar hiatus, which drains the maxillary sinus.
Sphenoid sinus infection Sinusitis affects about 1 in 8 adults in the United States, resulting in over 30 million annual diagnoses 3). Sinusitis, also called rhinosinusitis because the symptoms involve both the nose and the sinuses, affects about one in eight adults annually. For many, the inflammation starts when viruses or bacteria infect your sinuses (often during a cold), and begin to multiply. Part of the body’s reaction to the infection causes the sinus lining to swell, blocking the channels that drain the sinuses. This causes mucus and pus to fill up the nose and sinus cavities. For others, the symptoms and inflammation may be the result of the nose and sinuses reacting to other things in the environment, but not be an infection.
Because sinusitis simply means inflammation of the sinuses, the word alone includes a variety of similar problems. Acute sinusitis is when the symptoms occur for less than four weeks. A diagnosis of chronic sinusitis requires that the symptoms last longer than 12 weeks. Sometimes these are caused by the same thing, but often chronic and acute sinusitis are very different from each other. Your primary care provider or an ENT (ear, nose, and throat) specialist, or otolaryngologist, can help sort out what type of sinusitis you have and how to treat it. Recurrent acute sinusitis is when someone has four or more sinus infections (acute sinusitis) in one year but does not have symptoms in between those infections.
Four sinusitis classifications:
Acute rhinosinusitis: Sudden onset, lasting less than 4 weeks with complete resolution. Subacute rhinosinusitis: A continuum of acute rhinosinusitis but less than 12 weeks. Recurrent acute rhinosinusitis: Four or more episodes of acute, lasting at least 7 days each, in any 1-year period. Chronic rhinosinusitis: Signs of symptoms persist 12 weeks or longer. What causes sinusitis? Acute sinusitis is most commonly due to viruses or bacteria and is usually self-limiting. Approximately 90% of patients with colds have an element of viral sinusitis. Acute viral sinusitis is likely if you have been sick for less than 10 days and are not getting worse. Acute bacterial sinusitis is when you do not improve at all within 10 days of getting sick, or when you get worse within 10 days after beginning to get better. Those with atopy (allergy) commonly get sinusitis. It can be caused by allergens, irritants, viruses, fungi, and bacteria. Popular irritants are animal dander, polluted air, smoke, and dust.
Chronic sinusitis, however, is usually caused by prolonged inflammation, instead of a long infection. Infection can be a part of chronic sinusitis, especially when it worsens from time to time, but is not usually the main cause. The exact cause cannot always be determined; for some reason the nose and sinuses are overreacting to what they think is an infection.
There are higher rates of sinusitis in the South, Midwest, and among women. Children younger than 15 years of age and adults aged 25 to 64 years are affected the most 4).
Other risk factors or sinusitis include 5):
Anatomic defects such as septal deviations, polyps, conchae bullosa, other trauma and fractures involving the sinuses or the facial area surrounding them Impaired mucous transport from diseases such as cystic fibrosis, ciliary dyskinesia Immunodeficiency from chemotherapy, HIV, diabetes mellitus, etc. Body positioning, intensive care unit (ICU) patients due to prolonged supine positioning that compromises mucociliary clearance. Rhinitis medicamentosa, toxic rhinitis, nasal cocaine abuse, barotrauma, foreign bodies Prolonged oxygen use due to drying of mucosal lining Patients with nasogastric or nasotracheal tubes Are there any related conditions or complications?
Migraine headaches or tension headaches can cause symptoms of sinus pain or pressure. If you have sinus headaches without discolored drainage, talk to your primary care provider, or an ENT specialist, about the possibility of migraine headaches causing sinus pain or pressure and medications options for migraine treatment. Sometimes inflammation of the nasal cavity can also cause drainage and nasal congestion, but not involve your sinuses.
What are the symptoms of sinusitis? You have acute sinusitis when you have had cloudy or colored drainage from your nose for up to four weeks, plus one or more of the following symptoms:
Stuffy, congested, or blocked nose Pain, pressure, or fullness in the face, head, or around the eyes Long-lasting cold symptoms Symptoms that do not improve within 10 days of getting sick, or initially get better then worsen again You might have chronic sinusitis if you have at least two of the four symptoms note below for at least 12 weeks. An ENT specialist would also need to see polyps, pus, or thickened mucous in nose, or get a CT scan, to fully diagnose chronic sinusitis. Possible symptoms include:
Stuff congested, or blocked nose Pain, pressure or fullness in the face, head or around the eyes Thickened nasal drainage Loss of smell Sinusitis diagnosis No laboratory tests are indicated for acute uncomplicated sinusitis because the diagnosis is usually clinical. X-rays or CT scans of the sinuses are not necessary to diagnose uncomplicated sinusitis if you have the symptoms of sinusitis (discharge plus pressure or blockage). A plain sinus x-ray is most accurate for the maxillary, frontal, or sphenoid disease but is not useful for evaluating the anterior ethmoid cells or the ostiomeatal complex from which most sinus disease originates. Positive findings on plain films are air-fluid levels, sinus opacity, or mucosal thickening of 6 mm or more. Coronal CT at a thickness of 3 mm to 4 mm is the modality of choice. The CT findings suggestive of sinusitis are sinus opacification, air-fluid levels, sinus wall displacement, and 4 mm or greater mucosal thickening. Culture and biopsy are indicated for chronic bacterial and fungal sinusitis.
Sinusitis treatment options Sinusitis is treated differently based on the cause. Most cases of acute sinusitis, about 98 percent, are caused by a virus, not bacteria, and should not be treated with antibiotics. Acute viral sinusitis may be treated using pain relievers such as acetaminophen or ibuprofen, steroid nasal sprays, or salt water irrigation in the nose. These treatments are also good options for acute bacterial sinusitis. Most people get better naturally from acute bacterial sinusitis, called “watchful waiting,” but some patients with acute bacterial sinusitis may get better faster with an antibiotic.
Antibiotics: Use empirically and based on community patterns of resistance. Ten to 14 days of amoxicillin or amoxicillin-clavulanate is first-line treatment. In some communities, amoxicillin effectiveness is less than 70%. Trimethoprim-sulfamethoxazole well for some, but there is a higher rate of resistance. Failure of symptoms to resolve after 7 days of therapy should prompt one to switch to a broader spectrum agent, such as ten to fourteen days of augmentin, cefuroxime axetil, other second or third-generation cephalosporins, clindamycin alone or along with ciprofloxacin, sulfamethoxazole, a macrolide, or one of the fluoroquinolones. Metronidazole may be added to any one of these agents to increase anaerobic coverage. For chronic sinusitis, antibiotics should cover S. aureus and be effective against the higher incidence of beta-lactamase producing organisms that are common in chronic disease. If the patient is not improving after 5 to 7 days, add metronidazole or clindamycin. Treat for 3 to 6 weeks.
Frontal or sphenoid sinusitis with air-fluid levels may require hospitalization with intravenous (IV) antibiotics. Patients who are immunocompromised or are toxic appearing require admission. Fungal sinusitis is associated with high morbidity and mortality.
Sinusitis may extend to the bones and soft tissues of the face and orbits. Facial cellulitis, periorbital cellulitis, orbital abscess, and blindness can develop. Sinusitis can lead to intracranial complications such as cavernous sinus thrombosis, epidural or subdural empyema, and meningitis.
Chronic sinusitis is treated differently than acute sinusitis. Because chronic sinusitis is caused more by inflammation than infection, the treatments for chronic sinusitis aim to control the inflammation. Salt water nasal irrigation and/or nasal steroid sprays are the main treatments for the symptoms of chronic sinusitis. Antibiotics may sometimes be helpful but not always.
Other factors, including allergies, nasal polyps, asthma, and problems with the body’s ability to fight infections, can go along with sinusitis and make it worse unless they are also treated.
Antihistamines are only of benefit in early allergic sinusitis. Topical steroids are used to diminish nasal mucosal edema but are more efficacious in chronic and allergic sinusitis. Only start antibiotics if you strongly suspect bacterial disease.
Surgery Surgery is not recommended for acute sinusitis except in rare circumstances. Sometimes the sinus infection can spread to the eye, face, or brain; this would be considered an emergency, and surgery may be needed to reverse the infection and keep it from spreading.
For chronic sinusitis, surgery is an option when the symptoms cannot be controlled with medications and other treatments. The most common type of surgery for the sinuses is called endoscopic sinus surgery; a pencil-sized scope (endoscope) is used to see inside the nose and sinuses and guide the surgery. The surgery widens the natural drainage pathways between the sinuses and the nose, allowing mucus to get out of the sinuses and air to get in. Medications that are delivered into the nose and sinuses, like sprays and irrigations, can also get into the sinuses better after surgery.
Balloon sinus ostial dilation is a newer treatment option where an endoscope is also used, but instead of carefully removing the bone and tissue that may be blocking a sinus, a balloon is used to make the sinus openings bigger. Balloon dilation may not be appropriate for every type of chronic sinusitis and cannot be used on all of your sinuses, but can be helpful depending on your circumstances.
Sphenoid sinus surgery Sphenoidotomy is the surgical opening of the sphenoid sinus, is usually performed under general anesthesia. There are rare occasions when a surgeon may elect to perform a sphenoidotomy under local anesthesia in the operating suite or office setting. The indications for sphenoidotomy include acute and chronic sphenoid rhinosinusitis that is refractory to medical therapy; sphenoid mass or lesion; endonasal skull base or pituitary surgery; sphenoid cerebrospinal fluid leak repair; endonasal vidian neurectomy; and optic nerve or orbital decompression 6).
Sphenoid sinus surgery has no absolute contraindications. Relative contraindications include comorbidities that limit general anesthesia or conditions that increase the risk of bleeding. Care should also be taken when performing surgery on a hypoplastic sphenoid sinus or sphenoid sinus cavities with dehiscence of the internal carotid artery or optic nerve.
Procedure planning
Preoperative imaging should include noncontrast CT scanning of the sinuses to provide information about the bony architecture and pneumatization patterns of the sphenoid sinus. Other imaging studies may be advisable depending on the particular disease being managed. The characteristics that should be evaluated with regard to the sphenoid sinus prior to performing a sphenoidotomy include the following:
Pneumatization pattern in relation to the sella turcica (conchal, presellar, sellar, postsellar) Location of the natural ostium and its relationship to the superior turbinate (the image below demonstrates a right-sided sphenoid sinus natural ostium located medial to the superior turbinate). Location of the optic nerve, optic chiasm, and internal carotid artery with particular attention to presence or absence of bony dehiscence Presence or absence of a posterior ethmoid (Onodi) cell. Complication prevention
Prior to performing sphenoidotomy, the surgeon should carefully inspect the patient’s anatomic variants and extent of sinusitis. The surgeon should also use a standard approach that allows safe entrance into the sphenoid sinus. Stereotactic navigation should be considered, when warranted. In an effort to avoid severe complications, the surgeon should recognize potential pitfalls, such as cerebrospinal fluid leaks from inadvertent skull base injury, blindness from optic nerve injury, hemorrhage from the posterior septal branch of the sphenopalatine artery, or catastrophic hemorrhage from the internal carotid artery.
Regardless of the technique performed, care should be taken to avoid vital structures. The optic nerve may traverse laterally, and sometimes superiorly, in proximity to the sphenoid sinus or within an Onodi cell. Care should especially be taken to avoid disturbing the posterior wall of the sphenoid sinus, as this can risk injury to the carotid artery, optic chiasm, cavernous sinus, or pituitary gland. In addition, the surgeon should be aware that the posterior septal branch of the sphenopalatine artery traverses just inferior to the nature os of the sphenoid sinus; thus, removal of bone and mucosa inferiorly may cause inadvertent injury to this artery with resultant epistaxis. Some ways to avoid injury to this artery include elevating the mucosa off the bone or cauterizing the approximate site of the artery prior to performing inferior dissection. If bleeding is encountered secondary to this artery, it is fortunately readily controlled with monopolar or bipolar cauterization.
Sphenoid sinus surgery technique Several specific sphenoid procedures may be performed. Some procedures, including lavage of the sphenoid sinus and diagnostic sinuscopy, provide access to the sphenoid sinus without requiring surgical sphenoidotomy. Surgical dilation of the sphenoid ostium is a minimally invasive approach to widen the sinus ostium without removing tissue 7).
Sphenoidotomy is the surgical opening of the sphenoid sinus. Sphenoidotomy may be performed without or with tissue removal. The designation of “tissue removal” has been defined by the American Academy of Otolaryngology-Head and Neck Surgery as removal of material or tissue, not just suctioning of mucus or pus.
The techniques for endoscopic sphenoidotomy may be divided into (1) transethmoidal versus transnasal approach and (2) opening via the natural os versus through the anterior sinus wall.
The size limitations of the sphenoidotomy depend on the size of the sphenoid sinus. The optimal size of the sphenoidotomy is unknown; however, it is generally considered important to perform wider sphenoidotomies in obstructive sinonasal disease such as polyposis and allergic fungal sinusitis. Expanded endonasal approaches via the sphenoid sinus often require extended procedures, including concomitant posterior septectomy, removal of the intersinus septum, and drilling away a portion of the rostrum and inferior portion of the anterior sphenoid sinus wall.
Endoscopic Sphenoidotomy, Transnasal via the Natural Ostium Endoscopic transnasal sphenoidotomy without ethmoidectomy via the natural ostium can be considered in cases of isolated sphenoid sinus disease 8). This approach has the advantage of being minimally destructive of nasal mucosa and can result in shorter operative and recovery times; however, access to the sphenoidotomy site postoperatively may be limited because the ethmoid sinus cavity has not been opened.
A 30° nasal endoscope is often beneficial to provide visualization of the sphenoid sinus opening. Removal of part of the superior turbinate may be necessary to access the ostium and to facilitate postoperative care and inspection. The natural ostium of the sphenoid sinus usually lies just posterior to the superior turbinate. The anatomic landmarks that may be used to locate the natural ostium of the sphenoid sinus include the following 9):
Posterior to the superior turbinate in the sphenoethmoid recess; the natural ostium is medial to the superior turbinate in 80% of cases Approximately 6 cm from the nasal sill at an angle of 30° from the nasal cavity floor Approximately 1 cm above the superior extend of the choana At the approximate level of the maxillary sinus roof Once the sphenoid ostium is identified, it is enlarged using a sphenoid sinus mushroom punch or a small Kerrison punch. The contents within the sphenoid sinus are then cultured, biopsied, irrigated, or removed. Care should be taken to avoid manipulation of the posterior wall of the sphenoid sinus, which could risk injury to the internal carotid artery, optic nerve, or skull base.
Endoscopic Sphenoidotomy, Transethmoidal via the Natural Ostium Endoscopic transethmoidal sphenoidotomy is a sphenoidotomy performed through the passageway of an ethmoidectomy. This approach is the most commonly performed method, as it gives the widest view of the sphenoid sinus from lamina papyracea to rostrum. A total ethmoidectomy is first performed until the anterior face of the sphenoid sinus, skull base, and superior turbinate are identified. A decision can then be made to approach the sphenoid via the natural os or through a puncture into a thin section of bone of the anterior face of the sphenoid sinus. Although no comparison trials have evaluated these two methods, each has theoretical and anecdotal advantages and disadvantages.
Performing a sphenoidotomy via the natural os is theorized to limit postoperative recirculation of mucus and may be safer, as the sphenoid sinus is opened via a known opening in the sinus. In contrast, a sphenoidotomy via the anterior sinus wall avoids removing a potentially healthy superior turbinate and may lessen the risk of olfactory dysfunction. The comparative complication and patency rates between these two procedures are unknown.
A 0° nasal endoscope is typically used for the procedure. Angled endoscopes (30°, 45°, or 70°) are occasionally used to visualize the corners or floor of the large sphenoid sinus cavities once a sphenoidotomy has been performed. When identifying the natural ostium, the inferior one third to half of the superior turbinate is often resected using a straight thru-cutting forceps. It is not advisable to resect the superior turbinate too superiorly because of risks to olfactory dysfunction and skull base injury with cerebrospinal fluid leak. The natural ostium of the sphenoid sinus usually lies just posterior to the superior turbinate. The anatomic landmarks that may be used to locate the natural ostium of the sphenoid sinus include the following 10):
Posterior to the superior turbinate in the sphenoethmoid recess; the natural ostium is medial to the superior turbinate in 80% of cases Approximately 6 cm from the nasal sill at an angle of 30° from the nasal cavity floor Approximately 1 cm above the superior extend of the choana At the approximate level of the maxillary sinus roof A J-curette or image guidance probe are helpful to bluntly palpate and identify the os when it cannot be visualized initially 11). Once the natural os is identified, a straight mushroom punch, Kerrison punch, or other instrumentation may be used to enlarge the opening laterally and superiorly.
Endoscopic Sphenoidotomy, Transethmoidal via Anterior Sinus Wall Endoscopic transethmoidal sphenoidotomy via the anterior sinus wall avoids removing a potentially healthy superior turbinate and may lessen the risk of olfactory dysfunction.
A total ethmoidectomy is first performed until the anterior face of the sphenoid sinus, skull base, and superior turbinate are identified. A 0° nasal endoscope is typically used for this approach. Angled endoscopes (30°, 45°, or 70°) may be used to visualize the corners or the floor of the large sphenoid sinus cavities once a sphenoidotomy has been performed.
The superior turbinate is usually not resected unless the surgeon decides to incorporate the natural os. The image guidance system may be used to locate a safe location for entering the sinus. If no image guidance is available, the surgeon should choose a location that is somewhat inferior and medial with palpably evident thin bone to avoid skull base injury. A blunt sickle knife or J-curette is used to puncture through a thin section of bone in the anterior face of the sphenoid sinus. The sphenoid sinus mushroom punch, Kerrison punch, or other instrumentation can then be used to widen the sphenoidotomy.
Lavage of the sphenoid sinus The least invasive procedure of the sphenoid sinus is a lavage of the sphenoid sinus, in which the sphenoid sinus is accessed either via the natural opening or through the sphenoid sinus face. The sinus is irrigated with saline and aspirated. The contents can then be cultured or evaluated by a pathologist.
A nasal/sinus endoscopy with sphenoid sinuscopy A nasal/sinus endoscopy, diagnostic with sphenoid sinuscopy is a procedure in which a puncture is created or cannulation is performed of a nonsurgically opened ostium. The contents can then be irrigated, aspirated, cultured, or biopsied.
Nasal/Sinus Endoscopy, with dilation of sphenoid sinus ostium A nasal/sinus endoscopy with dilation of the sphenoid sinus ostium is procedure in which the sphenoid sinus ostium is dilated mechanically to allow improved drainage and access to the sphenoid sinus. The procedure can be performed in the office setting or the operating room. Topical anesthesia and decongestion is performed.
In an unoperated sinus, the natural ostium is typically identified medial to the superior turbinate. Depending on the style of catheter used, a probe or a wire is gently inserted into the ostium. Once the sinus is successfully cannulated, the dilation device or balloon is advanced into the sinus ostium. The balloon is then inflated to dilate the sinus ostium. The sinus contents may then be irrigated, aspirated, cultured, or biopsied.
Sphenoid sinus surgery risks The risks of endoscopic sphenoidotomy include, but are not limited to, the following 12):
Bleeding Infection Anesthetic risks Scarring Recurrence of disease Skull base injury, cerebrospinal fluid leak, and meningitis Eye or vision loss and orbital nerve or optic chiasm injury Carotid artery injury Postoperative ostial stenosis Mucocele formation Sphenoid sinus surgery recovery The postoperative management of a endoscopic sphenoidotomy is similar to that of other procedures in functional endoscopic sinus surgery. Patients are often asked to perform nasal saline irrigations or lavages several times a day. Postoperative antibiotics and oral corticosteroids are given per surgeon preference.
Patients are usually seen in clinic for nasal endoscopy with debridement at about 1-2 weeks after surgery. The debridement of crusts and blood clots, as well as the early identification of scar tissue, helps limit postoperative adhesions.
Sphenoid sinus surgery outcomes Sphenoidotomy appears efficacious based on case series studies 13). No prospective randomized controlled trials have evaluated sphenoidotomy.
† 성부와 성자와 성령의 이름으로 아멘. |
||||
|
태그
|
||||
