


매일미사
우리들의 묵상/체험
| 제목 | 21 02 06 토 평화방송 미사 요사이 빛의 생명과 특히 새 생명을 계속 주어 저의 죄의 상처가 없어 지고 있어 성장하고 발전하여 다스림의 감지가 어려움 | |||
|---|---|---|---|---|
작성자한영구

|
작성일2021-08-10 | 조회수2,868 | 추천수0 |
반대(2)
 신고
신고
|
|
성부와 성자와 성령의 이름으로 아멘. 흠숭 하올 우리 주 성체 예수 그리스도님, 오늘 2월 6일 성 바오로 미키와 동료 순교자들 기념일 토요일 평화방송 정오 미사를 선택하여 참례하였습니다. 미사가 시작되자 저의 두 눈 사이 콧날 양쪽 경사 끝 뼈에 머물러 만져주시면서 다스려주십니다. 두정엽 정수리에 머물러 만져주시면서 빛의 생명을 아래로 주시어 연결하여 다스려주십니다. 그러자 저의 아랫배에서 가스가 솟아올라 입으로 토해냈습니다. 의외로 빨리 토해냈습니다. 빛의 생명을 주시었는데 가스를 토해내자 제가 좀 판단하기가 어려웠습니다. 저의 생명을 점검하시는 것이 아니고 바로 벌집 굴과 연결하여 다스려주시어 가스를 토해내게 하여주신 것 같다고 상상하자, 그 가스가 소장에서 올라왔을 것 같다는 생각이 떠올랐습니다. 방귀가 나왔으면 직장에서 나온 것일 것입니다. 그리고 두정엽 정수리에서 약간 떨어진 전두엽 우뇌 오른쪽에 머물러 만져주시면서, 두 눈 사이 콧날 양쪽 경사 뼈에 머물러 연결하여 다스려주십니다. 벌집 굴을 열어 다스려주신다면 산소를 소장이나 S상 결장의 혈관 안으로 보내어 순환시키시어 다스려주시어 상처가 있는 곳에서 가스가 목구멍으로 나왔을 것입니다. 다음부터는 방귀가 나오면 직장이고 가스를 토해내면 S상 결장이나 소장에서 나온 것으로 판단하는 것이 맞을 것 같습니다. 미사가 진행되면서 저의 전두엽 우뇌의 아랫부위 오른쪽 눈썹 오른쪽 끝부분에 머물러 만져주시면서, 저의 물렁 코뼈 오른쪽 경사 끝 뼈에 머물러 두 곳을 연결하여 나비 굴을 열어 신경계와 연결하여 다스려주십니다. 저의 몸에 죄의 상처가 많이 없어져 태초의 생명으로 많이 되돌려졌다고 요사이 느끼고 있습니다. 지금 나비 굴과 연결하여 신경계를 다스려주십니다. 저의 오른쪽 귀 안에서 내이의 조직의 기관이 움직이는 소리가 들립니다. 이는 신경계를 다스려주시어 산소가 혈관 안으로 흘러들어 오른쪽 귀 안에 내이의 조직의 기관 안에서 그 산소 기압으로 활발하게 움직이어 고막의 안쪽을 울리는 소리가 들립니다. 오늘도‘영성체기도’에서 두 눈 사이 콧날 양쪽 경사 끝 뼈에 머물러 만져주시고, 두정엽 정수리에 머물러 만져주시어 빛의 생명을 주시고, 저의 심장박동 안에서 창조주 성부 하느님의 심장박동이 고동쳐주시어 그 고동이 양쪽 허파 윗부분 두 곳 박동 안에 퍼져나가 심장과 허파의 두 곳이 뻐근함을 느낍니다. 새 생명을 주십니다. 에펠탑 모양으로 빛의 생명과 새 생명을 주십니다. 그리고 두 눈 사이 콧날 양쪽 경사 뼈에 머물러 다스려주십니다. 그 뼈에 머물러 다스려주실 때 다스려주시는 목적이 무엇인지 판단하기 어려웠으나, 곧 벌집 굴을 연결하여 공기의 물질대사 습도와 온도를 최적의 상태로 유지하여주시고 허파의 기포(氣胞)로 산소를 크게 들여 마시어 그 산소가 혈관 안으로 들어가게 하여 그 산소가 피와 함께 혈관 속을 순환하여 저의 귀 안에 내이의 조직의 기관을 활발히 움직여 그 산소의 기압이 고막 안쪽을 울린다고 느껴집니다. 이어서 두 눈 사이 콧날 양쪽 경사 끝 뼈 위치에서 약간 아래로 내려온 위치에 머물러 만져주십니다. 아래로 내려온 위치는 물렁 코뼈 오른쪽 경사 끝 뼈에 머물러 만져주시면서, 이어서 전두엽 우뇌 오른쪽 눈썹 오른쪽 끝부분에 머물러 만져주시면서 두 곳을 연결하여 나비 굴을 열어 신경계를 다스려주십니다. 그 신경계를 다스려주시는데도 오른쪽 귀 안에서 활발히 움직이는 소리는 들리지 않습니다. 그리고 이번에는 저의 전두엽 우뇌 살갗 좌우 가운데 위치에서 약간 아래에 머물러 만져주시면서 아래로 내려오시어 이마뼈 굴 안에 머물러 나비 굴을 열어 그 굴 안의 신경계와 연결하여 다스려주시는 느낌입니다. 그리고 이어서는 저의 오른쪽 측두엽 안으로 아주 천천히 살금살금 들어오셨다가 나가십니다. 그 측두엽에 머물렀다 나가신 반응도 제가 느낄 수가 없었습니다. 그리고 이번에는 두정엽 정수리 가운데에서 약간 오른쪽으로 옮긴 두정엽 내의 위치에 머물러 만져주시면서, 수직으로 아래로 내려와 저의 그 물렁 코뼈 오른쪽 경사 끝 뼈와 연결하여 다스려주십니다. 이 역시 나비 굴을 열어 신경계를 연결하여 다스려주신다고 상상합니다. 그리고 중간에 두정엽 정수리에 머물러 빛의 생명을 주시고 심장과 허파 양쪽 윗부분 두 곳 안에 박동이 고동쳐주시어 심장과 허파 양쪽 윗부분 두 곳이 뻐근합니다. 새 생명을 주십니다. 그 빛의 생명과 새 생명을 받은, 상처가 있는 기관이 반응하여 뚜렷하게 움직이는 것을 느낄 수가 없으므로 어디를 다스려주시었는지도 기억하기 어렵습니다. 이는 요사이 저의 죄의 상처가 많이 없어졌으므로 과거처럼 민감하게 다스려주신 곳을 느끼지 못하는 것이라고 상상합니다. 그러나 성령님께서는 계속 전두엽 우뇌에서 위치를 옮겨가시면서 나비 굴을 열거나 혹은 코의 인두에 머물러 침의 물질대사를 다스려 침의 분비를 촉진하여 그 침이 대장이나 장기 안으로 또는 저의 귀 안으로 들어오게 다스려주신다고 상상합니다. 그러나 그 다스려주신 것을 제가 느낄 수가 없었습니다. 오늘 미사를 포함하여 미사 30분과 미사 후 20분 합계 50분 동안을 다스려주시었습니다. 다스림이 끝날 때는 저의 오른쪽 귀 안에서 내이의 조직이 움직이는 소리가 계속 들려왔습니다. 흠숭 하올 우리 주 성체 예수 그리스도님, 오늘 다스림으로 제가 점점 그 다스림의 효과와 성과를 판단하기가 어렵다고 느꼈습니다. 이는 저의 죄의 상처가 많이 없어졌기 때문이라고 생각합니다. 앞으로 그 다스려주시는 생명 지식을 제가 알기가 어려울 것으로 느꼈습니다. 이처럼 성장하고 발전한 저의 영혼과 몸과 오늘 다스려주시는 그 생명 지식을 아는 것이 더 어려워질 것과 이 모두를 주님께 바칩니다. 지극히 높으시고 지극히 거룩하신 하느님의 뜻으로 이 못난 작은 이를 다스려주시는 그 자체만으로도 너무너무 감사합니다. 하느님 뜻의 사랑으로 이 못난 작은 이를 이처럼 사랑하여주시어, 크게 성장하고 발전하게 하여주신 그 하느님 뜻의 사랑으로 하느님을 더욱더 사랑합니다. 아멘. 영광이 성부와 성자와 성령께 처음과 같이 이제 와 항상 영원히 아멘. 성부와 성자와 성령의 이름으로 아멘.
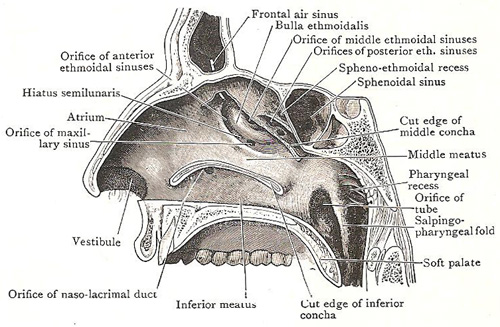 사진출처 : www.daviddarling.info/ Frontal air sinus 이마뼈 굴 안의 공기를 포함하는 공간 Bulla ethmoidalis 벌집 뼈의 물집- 수포(水泡), Orifice of middle ethmoidal sinuses 중간 벌집 굴의 구멍 Orifice of posterior ethmoidal sinuses 뒤 벌집 굴의 구멍 Spheno-ethmoidal recess 나비 굴과 벌집 굴의 움푹 들어간 곳 Sphenoidal sinus 나비 굴, 접형동 Cut edge of middle concha 가운데 비갑개의 자른 가장자리 Middle meatus 가운데 비갑개 Pharyngeal recess 인두에 움푹 들어간 곳 Orifice of tube (인두) 관(管)의 구멍 Salpingo- pharyngeal fold 유스타키오 관과 코의 인두를 연결하는 접어 포개진 곳 Soft palate 부드러운 입천장, 연구개(軟口蓋) Cut edge of inferior concha 아래 비갑개의 자른 가장자리 Inferior meatus 아래 비갑개 관(管- 대롱, 길, 구멍 관) Orfice of naso-lacrimal duct 비루관의 구멍 Vestibule 전정(前庭), (특히 내이(內耳)의) 미로(迷路) 전정. Orfice of maxillary sinus 위턱뼈 굴의 구멍 Atrium 심이(心耳); 고실(鼓室)《귀의》; 심방(心房) Hiatus semilunaris 반달 틈새. 사골포(篩骨胞)의 전하부에 있는 열공으로 전사골봉소(前篩骨蜂巢), 상악동(上顎洞) 때로 전두동(前頭洞)이 열공을 중계하여 중비동(中鼻洞)에 개구한다 Orifice anterior ethmoidal sinuses 앞쪽 벌집 굴의 구멍.
코 부비동
StatPearls [인터넷]. 해부학, 머리와 목, 코 부비동 Zachary J. Cappello ; Katrina Minutello ; Arthur B. 더블린 . 작가 정보 마지막 업데이트 : 2020 년 7 월 10 일 .
소개
비강은 대략 원통형의 중간 선의 공기 통로로, 비강 ala - 날개 -에서부터 뒤쪽으로 choana - 뒤 콧구멍 -까지 확장됩니다. 비강 중격에 의해 중간 선으로 나뉩니다. 각각의 측면에, 위턱뼈 굴이 옆면에 있으며, 이마뼈 굴, 벌집 굴, 나비 굴 순으로 앞쪽에서 뒷쪽으로,지붕 모양으로 덮여 있습니다. 단순 해 보이지만, 부비동 해부학은 복잡하고 세분화 된 공기 통로와 부비동을 연결하는 배수 통로로 구성됩니다.
이동 : 구조 및 기능 인간에게는 4 쌍의 부비동이 있습니다. 그들은 모두 pseudostratified - 여러겹 - 원주 상피와 일치합니다.
상악동 - 위턱뼈 굴 : 상악골의 눈 아래에 위치한 가장 큰 부비동. 전두동 - 이마뼈 굴 : 전두골 내 눈보다 위에 위치 사골동 - 벌집 굴 : 코와 눈 사이의 사 골 내에있는 여러 개의 분리 된 공기 세포에서 형성됨 접형동 - 나비 굴 : 나비 모양 뼈 안에 위치 부비동의 기능에 관한 토론이 활발하게 이루어지고 있습니다. 그렇지만 다음과 같은 여러가지 역할과 관련이 있습니다.
두개골의 상대적인 무게 감소 목소리의 공명 증가 안면 외상에 대한 완충제 제공 코의 급격한 온도 변화로부터 민감한 구조물을 단열 영감을 받은 공기를 가습 및 가열 면역 방어 부비동 해부학에 대한 강력한 이해를 개발하려면 부비동과 주변 구조의 해부학 적 관계를 이해하는 것도 중요합니다. 측면 비강 벽에는 부비동 해부학을 이해하는 데 중요한 많은 구조와 홈이 있습니다.
비갑개 뼈(鼻介骨)들 : 발기 성 점막으로 덮인 3 ~ 4 개의 뼈 선반은 내부 표면적을 증가시키는 역할을합니다.
도관-길-들 : 각 비갑개 아래에 세 개의 공간이 있습니다. 위의 도관은 접형 뼈와 후 사골동에 배액을 제공합니다. 가운데 도관은 전두엽, 전사 골, 상악동에 배액을 제공합니다. 아래 도관은 비루관의 구멍을 포함합니다.
갈골이 과정 : 점막 골막으로 덮여있는 사골 뼈의 낫 모양의 가늘고 뼈 부분으로, 사골의 내측과 중 비갑개의 측면
사골 깔대기- infundibulum : 이것은 상악, 전방 사골 및 전두동의 배액을 촉진하는 피라미드 형 공간입니다. uncinate 프로세스의 우수한 부착은 전두동 배액의 공간적 관계를 결정합니다 (다른 섹션에서 논의 됨).
반달모양의 열공(裂孔) - Semilunar hiatus : 이것은 사골의 깔대기(infundibulum)을 비우고 갈고리(uncinate) 과정과 사골 수포 사이에 위치하는 간격입니다
골반 복합체 - Osteomeatal complex (OMC : 상악동, 전두골 및 사골동의 골골을 포함하는 전방 사골을 나타내는 영역. 이것은 중간 비갑개 옆에 위치합니다. 분리 된 해부학 적 구조는 아니지만, 대신 중간 도미도, 갈고리(uncinate) 프로세스, 사골 깔대기(infundibulum), 앞 사골 세포 및 전방 사골, 상악 및 전두동의 골골을 포함하는 여러 중간 도관 구조의 모음입니다.
Nasal Fontanelles : 뼈가 존재하지 않는 측면 비강 벽 영역. 상악동의 자연 공공은 전방 천문에 있습니다.
상악동 - 위턱뼈 굴
상악동은 상악골의 눈 아래에 있습니다. 인접한 구조에는 비강 측벽, 안와 바닥 및 익 상구 개와를 포함하는 후 상악 벽이 포함됩니다. 상악동은 안와 아래 신경 (CN V2)에 의해 자극됩니다. 상악 및 안면 동맥은 부비동을 공급하고 상악 정맥은 정맥 배액을 공급합니다. 이미 언급했듯이 상악동은 사골 근으로 흘러 들어갑니다. 일반적으로 상악동 당 하나의 공공 만 있습니다. 그러나 사체 연구에 따르면 10 ~ 30 %는 보조 공을 가지고 있습니다. 성인기 상악동의 크기는 약 15mL로 가장 큰 부비동입니다.
전두동 - 이마뼈 굴
전두동은 안와보다 우월하고 전두골 내에 있습니다. 성인 단계의 일반적인 부피는 4 ~ 7mL입니다. 정면 부비동은 중간 도관을 통해 정면 홈으로 배수됩니다. 이전에 언급 한 바와 같이,이 배수는 부착에 따라 내측 또는 외측으로 가변적 일 수 있습니다. 전두동 혈관계는 안와 위 및 안와 위 동맥과 안과 및 안와 위 정맥으로 구성됩니다. 유사하게, 그것은 신경 분포가 안와 상 신경 (CNV1)에 의해 제공됩니다. 여러 해부학 적 공간 / 구조가 전두동 해부학에 중요합니다.
Frontal Recess : 전두동과 반월 틈새 사이의 배수 공간은 agger nasi 세포, lamina papyracea 및 중간 비갑개의 후벽에 의해 경계가 지정됩니다. Frontal sinus infundibulum : agger nasi 세포보다 우월한 정면 오목한 곳으로 배수되는 공간 정면 세포 : 정면 오목한 부분을 공기 중화시키는 전방 사골 세포. 이 세포는 폐색 또는 지속적인 부비동 질환을 유발할 수 있습니다. 그들은 agger nasi 세포보다 뒤쪽에 위치하며 Bent와 Kuhn으로 분류되는 4 가지 유형이 있습니다. I 형 : 단세포 위의 단세포이지만 전두동 바닥 아래 유형 II : agger nasi 위의 여러 세포, 전두동으로 확장 될 수 있음 유형 III : 전두동의 바닥을 통해 안와 상으로 확장되는 단일 큰 세포, 전방 테이블에 부착 유형 IV : 전두동 내에 포함 된 단일 분리 세포
접형동 - 나비 굴
접형동은 접형골 내 중앙 및 후방에 위치합니다. 그들은 상미도 내에 위치한 접형골 홈으로 배수됩니다. sphenopalatine 동맥은 부비동을 공급하고 정맥 배액은 상악 정맥을 통해 이루어집니다. 신경 분포는 부교감 신경과 CN V2로 구성된 sphenopalatine 신경에 의해 제공됩니다. 일반적인 성인 크기는 0.5 ~ 8mL입니다. 몇 가지 중요한 구조는 접형동과 밀접한 해부학 적 관계를 가지고 있습니다. 경동맥은 부비동의 측벽에 인접 해 있으며, 환자의 25 %에서이 부위에서 열이 발생합니다. 시신경은 또한 부비동의 측벽에 인접 해 있으며 개인의 최대 5 %에서 열화 될 수 있습니다.
사골동 - 벌집 굴
출생시 3 ~ 4 개의 세포가 있으며 성인이되면 10 ~ 15 개로 성장하여 총 부피는 2 ~ 3mL입니다. 그들은 눈 사이에 있습니다. 전방 사골은 중간 도미도의 사골 infundibulum으로 배수됩니다. 후방 사골동은 상부 도관 절에 위치한 접형골 홈으로 배수됩니다. 사골동은 각각 전방 및 후방 사골 동맥에 의해 공급됩니다. 이 동맥은 안 동맥의 가지로, 내 경동맥의 한 가지입니다. 이것은 가능한 CVA를 초래하는 ICA로 색전 물질의 역행 이동 가능성으로 인해 비출을 치료할 때 사골 동맥의 혈관 내 색전술을 피해야하기 때문에 실현해야 할 중요한 해부학 적 관계입니다. 사골동 정맥 배액은 상악 및 사골 정맥을 통해 이루어집니다. 전방 및 후방 사골 정맥은 신경 분포를 제공합니다. 복잡한 사골 미로는 발생 학적 전구체를 기반으로 일련의 라멜라로 축소 될 수 있습니다. 이 라멜라는 비스듬히 향하고 서로 평행하게 놓여 있습니다. 첫 번째 라멜라는 uncinate 프로세스입니다. 두 번째 박편은 사골 수포에 해당합니다. 세 번째 박편은 중비 갑 개의 기저 또는 지상 박편으로도 알려져 있습니다. 이 라멜라는 앞쪽과 뒤쪽 사골의 분할 역할을합니다. 앞쪽 부분은 crista ethmoidalis에 수직으로 삽입됩니다. 중간 부분은 lamina papyracea에 비스듬히 부착됩니다. 후부 1/3은 파피 라 시아 층에도 부착되지만 수평 방식으로 부착됩니다. 네 번째 박편은 상 비갑개입니다. agger nasi 세포는 전방 사골 세포의 가장 앞쪽에 있습니다. 그것은 측면 벽에 대한 중간 비갑개 부착보다 전방 및 우월한 것으로 발견됩니다. agger nasi 세포의 후벽은 정면 오목 부의 전벽을 형성합니다. 사골 수포는 infundibulum 위에있는 전방 사골 세포 중 가장 큰 세포입니다. 이 구조는 전방 사골 동맥이이 세포의 지붕을지나 가기 때문에 중요합니다. 이동 : 발생학 부비동의 발달은 ethmoturbinals로 알려진 임신 8 주째에 외측 비강 벽에 일련의 융기 또는 주름의 출현으로 예고됩니다. 처음에는 6 ~ 7 개의 폴드가 나타나지만 결국에는 회귀와 융합을 통해 3 ~ 4 개의 융기 만 지속됩니다.
첫 번째 ethmoturbinal : 인간의 초보적이고 불완전한 부분은 agger nasi 하강 부분을 형성하여 uncinate 과정을 형성합니다. 두 번째 ethmoturbinal : 중 비갑개 형성 세 번째 ethmoturbinal : 상 비갑개 형성 네 번째 및 다섯 번째 ethmoturbinals : 최고 비갑개를 형성하는 퓨즈 개발이 진행됨에 따라 이러한 ethmoturbinals 사이에 고랑이 형성되어 기초적인 고기와 움푹 들어간 곳이 형성됩니다.
전두동은 전두엽이 전두골로 전공 기화되어 발생합니다. 전두동은 5 ~ 6 세가 될 때까지 나타나지 않습니다. 접형동은 임신 3 개월 동안 발생합니다. 이 시간 동안 비점막은 연골 비강 캡슐의 뒤쪽 부분으로 침투하여 주머니 모양의 구멍을 형성합니다. 이 연골을 둘러싼 벽은 태아 발달 후기에 골화됩니다. 그런 다음 생후 2 년과 3 년 동안 연골이 재 흡수되고 구멍이 접 형체에 부착됩니다. 생후 6 년 또는 7 년이되면 접형동의 공기 화가 진행되고 12 년이되면 전 치상과 익상 돌기의 공기 화로 공기 화가 완료됩니다. 상악동은 자궁에서 처음으로 발생합니다. 상악동은 3 세와 7 세에서 18 세 사이에 성장하는 2 상 성장 패턴을 보여줍니다. 사골동은 출생시 3 ~ 4 개의 공기 세포로 구성됩니다. 그리고 개인이 성인이 될 때까지 1 ~ 15 개의 기포 세포로 구성됩니다.
이동 : 혈액 공급 및 림프관 상악동의 주요 동맥은 외부 경동맥의 한 가지 인 내부 상악 동맥입니다. 사골동과 전두동에는 사골동 위의 윤상 판을위한 수막 혈관과 전두엽 공기 세포의 후벽을 포함하여 다양한 혈액 공급이 있습니다. 접형동은 해면 내부 경동맥의 작은 가지에서 혈액 공급을 유도 할 수 있습니다. 드물게 내 경동맥의 동맥류가 접형동으로 침투하여 혈관 내 코일 링이 동맥류 제거에 선호되는 기술이 될 수 있습니다.
이동 : 신경 전두동 아래로 흐르는 주요 신경은 다섯 번째 뇌신경의 첫 번째 부분입니다. 상악동의 하 측면의 주요 신경은 다섯 번째 뇌신경의 두 번째 부분입니다. 이 신경은 감각 (주로 턱과 치아의 기술)과 운동 기능 (주로 저작 근육)을 모두 가지고있는 뇌신경 5의 세 번째 부분과 반대로 감각을 가지고 있지만 특정 운동 기능은 없습니다.
이동 : 근육 전두근은 전두골과 부비동 부위를 가로 지르며 표정 메커니즘의 일부입니다. 입술의 거근 근육은 상악동 위에 고정되어 있습니다. 상악의 광대뼈 돌출부는 턱의 강력한 폐쇄 인 안마 근의 고정 부분입니다.
이동 : 생리적 변형 비강 해부학은 개인마다 크게 다릅니다. 특정 해부학 적 변형은 비교적 일반적입니다. 이러한 변화는 비 부비동염으로 이어지는 osteomeatal complex의 기계적 막힘에 기여할 수 있습니다.
Concha bullosa는 중비 갑 개의 통기로 정의됩니다. 이 변형은 일방적이거나 양자적일 수 있습니다. 큰 경우, 중 비갑개에있는 concha bullosa는 중도 또는 infundibulum의 폐쇄로 이어질 수 있습니다.
비 중격 이탈은 비 연골 중격의 비대칭 굴곡입니다. 이러한 굴복은 중간 비갑개를 측면 방식으로 압축 할 수 있으며, 이로 인해 중도의 협착이 발생할 수 있습니다. 이 변이는 종종 선천적이지만 비강 외상에 이차적 일 수도 있습니다.
중간 비갑개는 일반적으로 비강 중격을 향해 중앙으로 휘어집니다. 그러나 비갑개가 옆으로 구부러지면 그 결과로 생긴 해부학 적 변형은 역설적 중 비갑개로 알려져 있습니다. 이러한 변종은 비강, 중도, 또는 뇌관을 좁히거나 막을 수 있습니다.
uncinate 프로세스는 개별 환자간에 여러 변형이있는 구조입니다. uncinate 프로세스의 우수한 부착에는 정면 오목 부 및 배수의 해부학 적 구성을 결정하는 데 도움이되는 세 가지 주요 변형이 있습니다.
파피 라 세아 또는 사골 수포에 부착하기 위해 옆으로 확장되는 uncinate 프로세스, infundibulum의 말단 오목 부를 형성하고, 앞 오목한 부분이 중간 도관으로 직접 열립니다. 내측으로 확장되어 중비 갑 개의 측면에 부착되는 미각 과정 두개골 기저에 직접 부착되도록 내측 및 우월하게 확장되는 uncinate 프로세스. 80 %의 시간에서 uncinate는 lamina papyracea에 부착되어 uncinate의 내측에있는 전두동 배액을 일으키고, uncinate의 20 %는 uncinate가 두개골 기저 또는 중 비갑개에 부착하여 uncinate의 측면 배액을 초래합니다. Haller 세포는 상악동 지붕의 내 측면 위로 측면으로 확장되는 사골 형 공기 세포입니다. 충분히 크면 밑바닥이 좁아 질 수 있습니다. Onodi 세포는 후방 사골 세포의 측면 및 후방 확장입니다. 접형동 주위의 수평 격막은 그들을 묘사합니다. 중요한 것은 이러한 세포가 시신 경관을 둘러싸고있어 수술 중 시신경 손상 위험을 증가시킬 수 있다는 것입니다.
마지막으로, 사골 지붕의 높이는 환자마다 다를 수 있으며 동일한 환자의 양쪽에 따라 다를 수 있습니다. 환자의 사골 지붕 높이가 비대칭 인 경우 FESS 중 두개 내 침투 위험이 더 높습니다.
이것은 sinonasal 해부학에서 볼 수있는 해부학 적 변이 중 일부에 불과합니다. 가장 일반적인 변형을 나타내지 만, 3 차원 해부학에 대한 건전한 이해의 중요성은 안전하고 효과적인 내시경 부비동 수술에 가장 중요합니다.
이동 : 외과 적 고려 사항 부비동염의 염증성 질환 치료에는 의학적 치료와 외과 적 치료가 모두 포함됩니다. 수술 관리를 고려할 때 만성 부비동염에 대한 몇 가지 일반적인 지침이 있습니다.
점막 골막을 보존하고 노출 된 뼈를 남기지 않도록 노력하십시오 질병 부위의 뼈 파티션과 골절을 가능한 한 완전히 제거하십시오. 가능한 경우 해부를 질병의 범위를 넘어서 한 단계 확장 가능하면 중 비갑개를 보존하십시오 이동 : 임상 적 의의 부비동은 염증과 감염에 취약합니다. 부비동이 분비물이나 덩어리로 막히면 점액의 배출이 중단되고 부비동염이 발생할 수 있습니다. 상악동은 치아 또는 잇몸의 모든 과정에서 발생할 수 있습니다. 전두동과 상악동이 알레르기와 관련이있을 수 있습니다. 원인에 따라 부비동염은 코르티코 스테로이드, 충혈 완화제, 비강 관개 및 수분 공급으로 치료됩니다. 배액을 향상시키기 위해 드물게 외과 적 개입이 필요할 수 있습니다.
부비동의 악성 종양은 드뭅니다. 대부분의 암은 상악동에서 발생하며 여성보다 남성에서 더 흔합니다. 상악동 악성 종양은 45 세에서 70 세 사이에 발생하며 가장 흔한 것은 육종입니다. 전이는 드물지만 이러한 악성 종양은 국소 침습적이며 파괴적입니다. 대부분의 경우 진단이 지연되고 예후가 좋지 않습니다.
급성 비 부비동염 (ARS)과 만성 비 부비동염 (CRS)은 모두 코와 부비동염의 증상적인 염증으로 정의됩니다. 2는 불만 제기 기간에 따라 구별됩니다. 일반적으로 급성 비 부비동염은 전염성 질환으로 널리 간주됩니다. 반면에 만성 비 부비동염은 일반적으로 염증성 질환으로 정의됩니다. ARS에서 근본적인 원인은 일반적으로 바이러스 또는 박테리아이며 때로는 곰팡이입니다. ARS의 병인은 감염에 이은 조직 침입을 수반합니다.
가장 널리 사용되는 분류 시스템은 비강 내시경 검사를 기반으로 CRS를 비강 폴립 (각각 CRSwNP 및 CRSsNP)이있는 CRS와없는 CRS로 구분합니다. 원래, CRSsNP는 ARS의 불완전한 해결로 이어지는 지속적인 염증을 특징으로하는 질병 과정이라고 느꼈습니다. 반면 CRSwNP는 아마도 아토피와 관련된 원인이 불분명 한 비 감염성 질병 과정으로 느껴졌다. 대신 현재 연구에 따르면 두 가지 형태의 CRS의 병인과 병인이 훨씬 더 복잡하다는 것이 밝혀졌습니다.
이동 : 질문 이 주제에 대한 무료 객관식 질문에 액세스하려면 여기를 클릭하십시오.
저작권 © 2020, StatPearls Publishing LLC.
Anatomy, Head and Neck, Nose Paranasal Sinuses Zachary J. Cappello; Katrina Minutello; Arthur B. Dublin.
Author Information Last Update: July 10, 2020. 저작권 © 2020, StatPearls Publishing LLC.
Go to: Introduction The nasal cavity is a roughly cylindrical, midline, airway passage that extends from the nasal ala anteriorly to the choana posteriorly. It is divided in the midline by the nasal septum. On each side, it is flanked by the maxillary sinuses, and roofed by the frontal, ethmoid, and sphenoid sinuses, in an anterior to posterior fashion. While seemingly simple, sinonasal anatomy is composed of intricate and subdivided air passages and drainage pathways that connect the sinuses.
Go to: Structure and Function There are 4 paired sinuses in humans. They are all in line with pseudostratified columnar epithelium.
The maxillary sinuses: Largest of the paranasal sinuses, located under the eyes in the maxillary bones. The frontal sinuses: Located superior to the eyes within the frontal bone The ethmoid sinuses: Formed from several discrete air cells within the ethmoid bone between the nose and eyed The sphenoid sinuses: Located within the sphenoid bone The function of the paranasal sinuses is debated. However, they are implicated in several roles:
Decreasing the relative weight of the skull Increasing the resonance of the voice Providing a buffer against facial trauma Insulating sensitive structures from rapid temperature fluctuations in the nose Humidifying and heating inspired air Immunological defense To develop a strong understanding of paranasal sinus anatomy, it is also important to understand the anatomical relationships of the sinuses to surrounding structures. The lateral nasal wall contains many structures and recesses that are important for understanding paranasal sinus anatomy.
Turbinates: Three to 4 bony shelves covered by erectile mucosa, serve to increase the interior surface area Meatuses: Three spaces located beneath each turbinate. The superior meatus provides drainage for the sphenoid and posterior ethmoid sinuses. The middle meatus provides drainage for the frontal, anterior ethmoid, and maxillary sinuses. The inferior meatus contains the orifice of the nasolacrimal duct Uncinate process: A sickle-shaped, thin, bony part of the ethmoid bone, covered by mucoperiosteum, medial to the ethmoid infundibulum and lateral to the middle turbinate Ethmoid infundibulum: This is a pyramidal space facilitating drainage of the maxillary, anterior ethmoid, and frontal sinuses. The superior attachment of the uncinate process determines the spatial relationship of the frontal sinus drainage (discussed in another section) Semilunar hiatus: This is a gap that empties the ethmoid infundibulum and is located between the uncinate process and the ethmoid bulla Osteomeatal complex (OMC): Region referring to the anterior ethmoids containing the ostia of the maxillary, frontal, and ethmoid sinuses. This is located lateral to the middle turbinate. While not a discrete anatomic structure, it is instead a collection of several middle meatus structures including the middle meatus, uncinate process, ethmoid infundibulum, anterior ethmoid cells, and ostia of the anterior ethmoid, maxillary, and frontal sinuses. Nasal Fontanelles: Area of the lateral nasal wall where no bone exists. The natural ostium of the maxillary sinus is located in the anterior fontanelle. Maxillary Sinus
The maxillary sinus is located under the eyes in the maxillary bone. Adjacent structures include the lateral nasal wall, the orbital floor, and the posterior maxillary wall which contains the pterygopalatine fossa. The maxillary sinus is innervated by the infraorbital nerve (CN V2). The maxillary and facial arteries supply the sinus, and the maxillary vein supplies venous drainage. As mentioned already, the maxillary sinus drains into the ethmoid infundibulum. There is typically only one ostium per maxillary sinus; however, cadaver studies have shown 10% to 30% have an accessory ostium. The size of the maxillary sinus at adult stage is approximately 15 mL, making it the largest paranasal sinus.
Frontal Sinus
The frontal sinus is located superior to the orbit and within the frontal bone. The typical volume at the adult stage is 4 to 7 mL. The frontal sinus drains into the frontal recess via the middle meatus. As noted previously, this drainage can be variable, either medial or lateral to the uncinate, depending on its attachment. The frontal sinus vasculature consists of the supraorbital and supratrochlear arteries and ophthalmic and supraorbital veins. Similarly, it's innervation is provided by the supraorbital and supratrochlear nerves (CNV1). Several anatomical spaces/structures are important to frontal sinus anatomy:
Frontal recess: Drainage space between the frontal sinus and semilunar hiatus that is bounded by the posterior wall of the agger nasi cell, lamina papyracea, and the middle turbinate. Frontal sinus infundibulum: Space that drains into the frontal recess that is located superior to the agger nasi cells Frontal cells: anterior ethmoid cells that pneumatize the frontal recess. These cells may cause obstruction or persistent sinus disease. They are located posterior and superior to the agger nasi cell, and there are 4 types as classified by Bent and Kuhn: Type I: Single cell above the agger nasi cell but below the floor of the frontal sinus Type II: Multiple cells above the agger nasi, may extend into the frontal sinus Type III: Single large cell that extends supraorbitally through the floor of the frontal sinus, attaches to the anterior table Type IV: Single isolated cell that is contained within the frontal sinus Sphenoid Sinus
The sphenoid sinuses are located centrally and posteriorly within the sphenoid bone. They drain into the sphenoethmoidal recess located within the superior meatus. The sphenopalatine artery supplies the sinus, and venous drainage is via the maxillary vein. Innervation is provided by the sphenopalatine nerve, which is comprised of parasympathetic fibers and CN V2. The typical adult size is 0.5 to 8 mL. Several important structures have a close anatomical relationship to the sphenoid sinus. The carotid artery is located adjacent to the lateral wall of the sinus, and in 25% of patients, it is dehiscent in this area. The optic nerve is also located adjacent to the lateral wall of the sinus and can be dehiscent in up to 5% of individuals.
Ethmoid Sinuses
There are 3 to 4 cells at birth and develop into 10 to 15 by adulthood for a total volume of 2 to 3 mL. They are located between the eyes. The anterior ethmoids drain into the ethmoid infundibulum, in the middle meatus. The posterior ethmoid sinuses drain into the sphenoethmoidal recess located in the superior meatus. The ethmoid sinuses are supplied by the anterior and posterior ethmoid arteries, respectively. These arteries are branches of the ophthalmic artery, which is a branch off of the internal carotid artery. This is an important anatomical relationship to realize because endovascular embolization of the ethmoid arteries should be avoided when treating epistaxis due to the possibility of retrograde movement of the embolization material into the ICA resulting in possible CVA. Ethmoid sinus venous drainage is by the maxillary and ethmoid veins. The anterior and posterior ethmoid veins provide innervation. The complex ethmoidal labyrinth can be reduced into a series of lamellae based on embryologic precursors. These lamellae are obliquely oriented and lie parallel to each other. The first lamella is the uncinate process. The second lamella corresponds to the ethmoid bulla. The third lamella is also known as the basal or ground lamella of the middle turbinate. This lamella serves as the division of the anterior and posterior ethmoids. The anterior part inserts vertically into the crista ethmoidalis. The middle portion attaches obliquely into the lamina papyracea. The posterior third attaches to the lamina papyracea as well but in a horizontal fashion. The fourth lamella is the superior turbinate. The agger nasi cell is the most anterior of the anterior ethmoid cells. It is found anterior and superior to the middle turbinate attachment to the lateral wall. The posterior wall of the agger nasi cell forms the anterior wall of the frontal recess. The ethmoid bulla is the largest of the anterior ethmoid cells that lies above the infundibulum. This structure is important because the anterior ethmoid artery courses over the roof of this cell. Go to: Embryology Development of the paranasal sinuses is heralded by the appearance of a series of ridges or folds on the lateral nasal wall at approximately the eighth week of gestation, known as the ethmoturbinals. Six to 7 folds emerge initially, but eventually, only 3 to 4 ridges persist through regression and fusion.
First ethmoturbinal: rudimentary and incomplete in humans ascending portion forms the agger nasi descending portion forms the uncinate process Second ethmoturbinal: Forms the middle turbinate Third ethmoturbinal: Forms the superior turbinate Fourth and fifth ethmoturbinals: Fuse to form the supreme turbinate As development progresses, furrows form between these ethmoturbinals, which leads to the establishment of rudimentary meati and recesses.
The frontal sinus originates from anterior pneumatization of the frontal recess into the frontal bone. The frontal sinus does not appear until the age of 5 to 6 years old. The sphenoid sinus develops during the third month of gestation. During this time, the nasal mucosa invaginates into the posterior portion of the cartilaginous nasal capsule to form a pouch-like cavity. The wall surrounding this cartilage is ossified in the later months of fetal development. Then, during the second and third year of life, the cartilage is resorbed, and the cavity becomes attached to the body of the sphenoid. By the sixth or seventh year of life, pneumatization of the sphenoid sinus progresses, and by the 12th year, the pneumatization is complete with pneumatization of the anterior clinoids and pterygoid process. The maxillary sinus is the first to develop in utero. The maxillary sinus shows a biphasic growth pattern, with growth at 3 and 7 to 18 years of age. The ethmoid sinuses are comprised of 3 to 4 air cells at birth. And by the time an individual reaches adulthood, they consist of 1 to 15 aerated cells.
Go to: Blood Supply and Lymphatics The major artery of the maxillary sinus is the internal maxillary artery, a branch of the external carotid artery. The ethmoid and frontal sinuses have a variety of blood supplies, including meningeal vessels for the cribriform plate above the ethmoid sinuses, as well as the posterior wall of the frontal air cells. The sphenoid sinuses may derive blood supply from small branches of the cavernous internal carotid arteries. Rarely, an aneurysm of the internal carotid artery may invaginate into the sphenoid sinus, making endovascular coiling the preferred technique for aneurysm obliteration.
Go to: Nerves The major nerve running below the frontal sinus is the first division of the fifth cranial nerve. The major nerve of the inferior aspect of the maxillary sinus is the second division of the fifth cranial nerve. This nerve has sensory but no specific motor functions, as opposed to the third division of cranial nerve five, the latter of which has both sensory (primarily skill of the jaw and the teeth) and motor functions (primarily muscles of mastication).
Go to: Muscles The frontalis muscle runs over the frontal skull and sinus region and is part of the mechanism of facial expression. The levator muscles of the lips are anchored over the maxillary sinuses. The zygomatic projection of the maxilla is part of the anchorage of the masseter muscle, a powerful closure of the jaw.
Go to: Physiologic Variants Nasal anatomy differs significantly among individuals; certain anatomic variations are relatively common. The variations may contribute to mechanical obstruction of the osteomeatal complex leading to rhinosinusitis.
Concha bullosa is defined as aeration of the middle turbinate. This variation can be either unilateral or bilateral. If large, a concha bullosa in the middle turbinate may lead to obstruction of the middle meatus or infundibulum.
The nasal septal deviation is an asymmetric bowing of the nasal cartilaginous septum. Such a bowing may compress the middle turbinate in a lateral fashion, which may lead to narrowing of the middle meatus. This variation is often congenital, but may also be secondary to nasal trauma.
The middle turbinate usually curves medially toward the nasal septum. However, when the turbinate curves laterally, the resultant anatomic variant is known as a paradoxical middle turbinate. Such a variant can narrow or obstruct the nasal cavity, middle meatus, or infundibulum.
The uncinate process is a structure that has multiple variations between individual patients. The superior attachment of the uncinate process has three major variations that help determine the anatomic configuration of the frontal recess and its drainage:
An uncinate process that extends laterally to attach to the lamina papyracea or the ethmoid bulla, forming a terminal recess of the infundibulum with the frontal recess opening directly into the middle meatus An uncinate process that extends medially and attaches to the lateral surface of the middle turbinate, with the frontal recess draining into the infundibulum An uncinate process that extends medially and superiorly to directly attached to the skull base, with the frontal recess draining into the infundibulum Eighty percent of the time, the uncinate attaches to the lamina papyracea resulting in frontal sinus drainage medial to the uncinate, while 20% of the time, the uncinate attaches to either the skull base or middle turbinate, resulting in drainage lateral to the uncinate. Haller cells are ethmoid air cells that extend laterally over the medial aspect of the roof of the maxillary sinus. If large enough, they may cause narrowing of the infundibulum. Onodi cells are lateral and posterior extensions of the posterior ethmoid cells. Horizontal septations around the sphenoid sinus delineate them. Importantly, these cells may surround the optic nerve tract, which can increase the risk of injury to the optic nerve during surgery.
Lastly, the height of the ethmoid roof can vary between patients and vary between each side in the same patient. When there is asymmetry of ethmoid roof height in a patient, the risk of intracranial penetration during FESS is higher.
These are only a few of the anatomic variations seen in sinonasal anatomy. While they represent the most common variations, the importance of having a sound understanding of the 3-dimensional anatomy is paramount to safe and effective endoscopic sinus surgery.
Go to: Surgical Considerations Treatment of inflammatory disease of the paranasal sinuses involves both medical therapy and surgical treatment. There are several general guidelines for chronic sinusitis when considering surgical management:
Preserve the mucoperiosteum and try not to leave the exposed bone Remove bony partitions and any osteitic bone in the area of disease as completely as possible Extend the dissection one step beyond the extent of disease if possible Preserve the middle turbinate if possible Go to: Clinical Significance Paranasal sinuses are prone to inflammation and infection. If the paranasal sinuses become blocked from secretions or a mass, the drainage of mucus is interrupted, and sinusitis can result. The maxillary sinus may be involved from any process in the teeth or the gums. The frontal and maxillary sinuses may be involved in allergies. Depending on the cause, sinusitis is treated with corticosteroids, decongestant, nasal irrigation, and hydration. Rarely surgical intervention may be required to enhance drainage.
Malignancies of the paranasal sinuses are rare. The majority of cancers occur in the maxillary sinus and are more common in men than women. Maxillary sinus malignancies occur between ages 45 to 70, and the most frequent is a sarcoma. Even though metastases are rare, these malignancies are locally invasive and destructive. Diagnosis in most cases is delayed, and the prognosis is poor.
Acute rhinosinusitis (ARS) and chronic rhinosinusitis (CRS) are both defined as symptomatic inflammation of the nose and paranasal sinuses. The 2 are distinguished based on the duration of the complaints. Generally speaking, acute rhinosinusitis is widely considered to be an infectious disorder. On the other hand, chronic rhinosinusitis is typically defined as an inflammatory disorder. In ARS, the underlying etiology is typically viral or bacterial, and occasionally fungal. The pathogenesis of ARS involves infection followed by tissue invasion.
The most widely accepted classification system divides CRS into CRS with and without nasal polyps (CRSwNP and CRSsNP, respectively) based on nasal endoscopy. Originally, it was felt that CRSsNP was a disease process characterized by persistent inflammation that led to incomplete resolution of ARS. CRSwNP, on the other hand, was felt to be a noninfectious disease process with unclear etiology, perhaps related to atopy. Current research has instead revealed that the etiology and pathogenesis of either form of CRS is much more complex.
† 성부와 성자와 성령의 이름으로 아멘. |
||||
|
태그
|
||||
